Mamdouh 🇸🇦 retweetledi

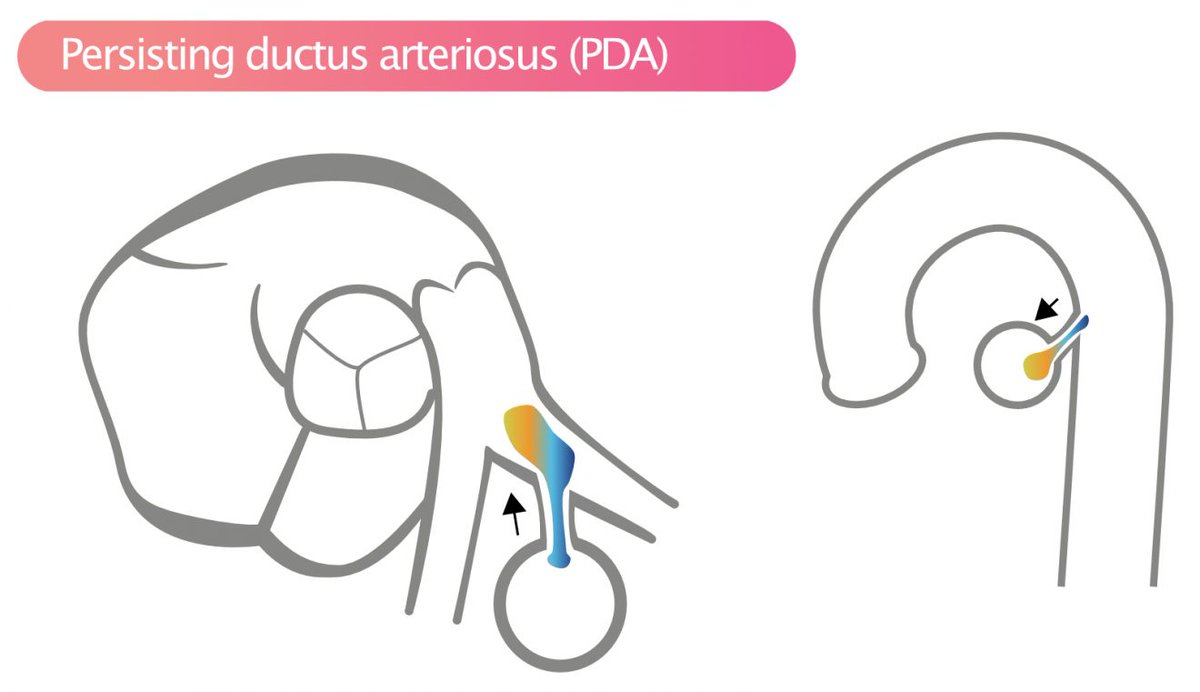
1M, Native juxtaductal (isthmic) CoA (immediately distal to LSCA)+BAV+PDA
📌Classic, not a diffuse arch Hypoplasia @AEPCcongenital @ASE360
@iamritu @CASivaram1 @alex1708ander @SIwa23288585 @echoleolopez @loomba_rohit @alexsfelixecho @swatigar @argulian @sujithsp @cardiopedhnn
English