DESTINY-Breast11 #ESMO25 🧬
Neoadjuvant T-DXd-THP vs ddAC-THP in high-risk HER2+ eBC:
pCR 67.3 vs 56.3 % (+11.2%, p = 0.003)
Grade ≥3 AE 37.5 vs 55.8 %
LVEF 1.9 vs 9 %
ILD 4.4 vs 5.1 %
Early EFS HR 0.56 (immature).
➡️ Better efficacy + safety, anthracycline-free option.
But pCR ≠ EFS ?? — needs mature follow-up.
Also cost factor ??
What to give on relapse ?
Surprised to see more ILD IN NON TDXD ARM ?
@myESMO#esmo2025@OncoAlert@OncBrothers
🚨 AURIGA Trial (NDMM post-ASCT)
💊 Maintenance: Dara+Len vs Len
MRD-neg @10⁻⁵: 61% vs 29%
MRD-neg @10⁻⁶: 36% vs 14%
Sustained MRD-neg (12 mo): 30% vs 8%
3-yr PFS: 77% vs 61% (HR 0.55)
OS (immature): 95% vs 91%
⚠️ Slight ↑ G3/4 infections, but overall manageable safety.
📌 Message: Adding Daratumumab to Len maintenance post-ASCT deepens MRD responses → translates into longer PFS, with OS trend favoring combo.
#Oncotwitter#Hematology#Myeloma@Myeloma_Society@Annals_Oncology
Tagrisso® (AstraZeneca) is the only version with approval from stringent regulators (US FDA/EMA/etc.) and clinical-trial–level, lot-to-lot oversight. Bangladesh/Bhutan “generics” (e.g., Beacon Tagrix®, Incepta Osicent®) are made under Bangladesh’s TRIPS waiver and are locally approved but not approved by US FDA/EMA; public, regulator-reviewed bioequivalence data aren’t available. So reliability is unknown/variable compared with Tagrisso, and depends entirely on the specific manufacturer’s GMP and the integrity of your supply chain.
@BSBaiims Sir, could you kindly guide about the authenticity and clinical reliability of Osimertinib 80mg from Bangladesh (Everest Pharma, ‘Osimert’) and Bhutan (Azista, ‘OsiTab’)? patients are coming across these versions in India through pharmacies, but we are unsure if they are genuine
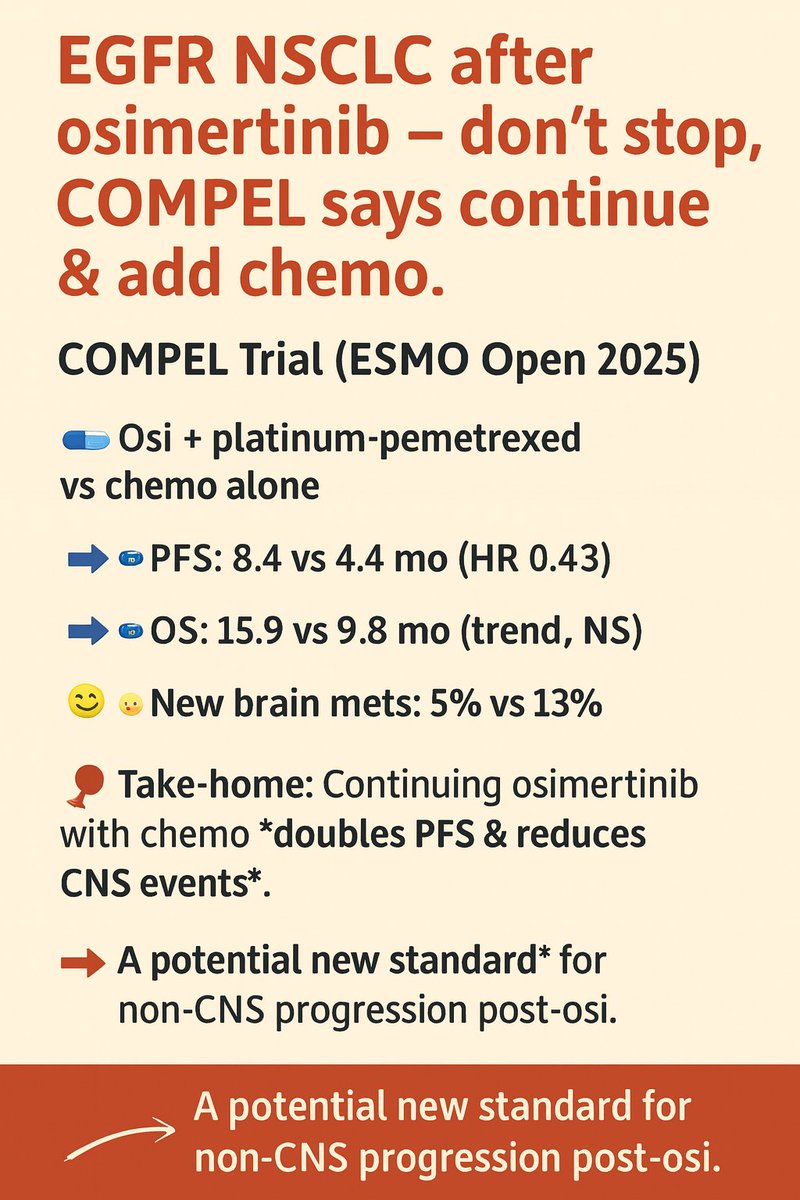
“EGFR NSCLC after osimertinib — don’t stop, COMPEL says continue & add chemo”
COMPEL Trial (ESMO Open 2025)
Post-progression strategy in EGFR-mutant NSCLC (non-CNS PD after 1L osimertinib):
🔹 Osi + platinum-pemetrexed vs chemo alone
➡️ PFS: 8.4 vs 4.4 mo (HR 0.43)
➡️ OS: 15.9 vs 9.8 mo (trend, NS)
➡️ New brain mets: 5% vs 13%
➡️ Safety: manageable, no new signals
📌 Take-home: Continuing osimertinib with chemo doubles PFS & reduces CNS events.
→ A potential new standard for non-CNS progression post-osi.
@Annals_Oncology@ESMO_Open@myESMO
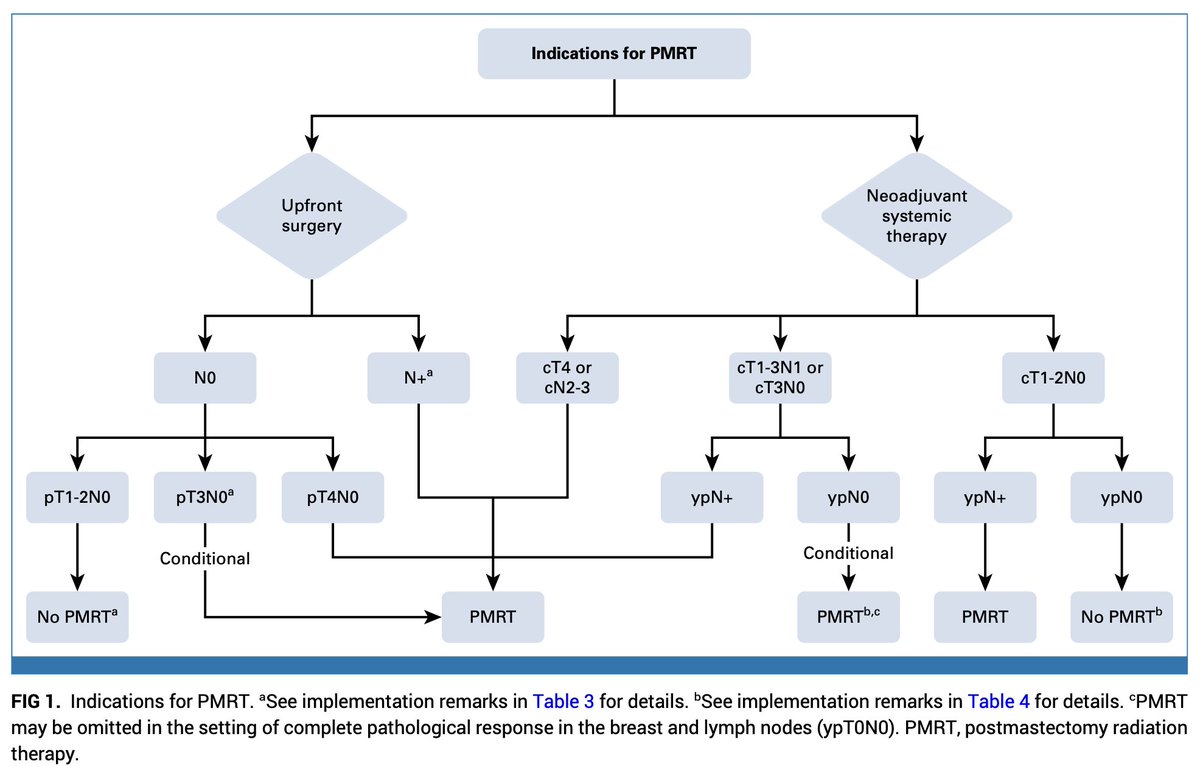
Postmastectomy Radiation Therapy: An ASTRO-ASCO-SSO Clinical Practice Guideline-2025
PMRT in ≥4 LN+, T4, residual ypN+; consider in cN1→ypN0 or T3N0; omit in T1-2N0 low-risk.
Hypofractionation is SoC, IMRT & DIBH↓ cardiopulmonary toxicity.
ascopubs.org/doi/10.1200/JC…@OncoAlert
🚨 Cancer Risk in Inborn Errors of Immunity ≈ 40× Higher than General Population!
Cancer frequency in IEI: 12% (≈40× higher than general population, 0.29%)
Most common subtype (absolute cases): CVID – 1,284 cases
Highest relative risk:
Nijmegen Breakage Syndrome (NBS1) – 50.5% cancer incidence
ATM deficiency – high risk, poor outcomes
Fanconi anemia – strongly linked to cancer
X-linked lymphoproliferative (XLP) syndrome – high cancer burden
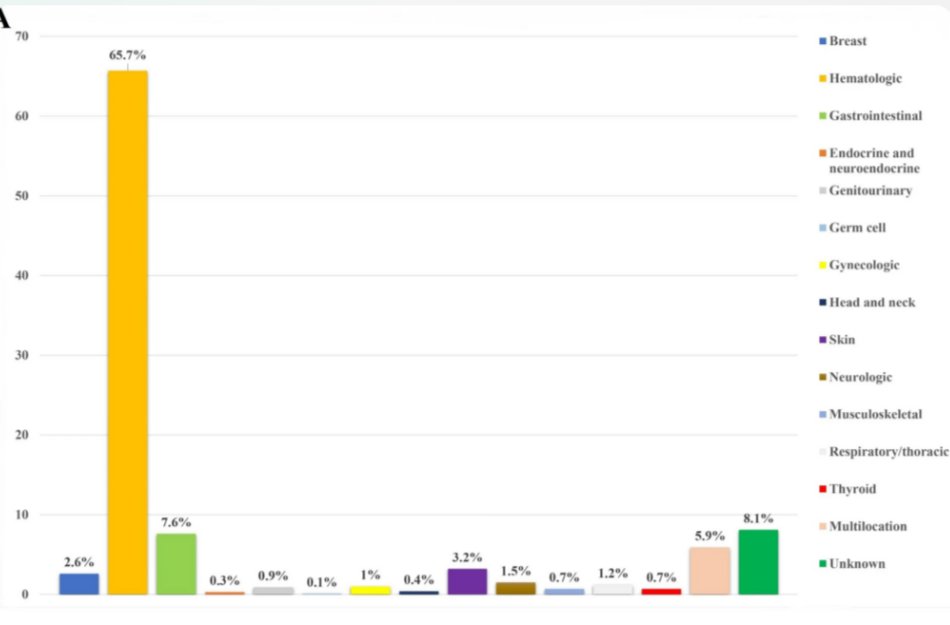
🎯 Cancer Types
Hematologic malignancies (65.7%)
Most frequent: Diffuse Large B-cell Lymphoma (DLBCL)
Solid tumors:
Digestive tract (stomach, colorectum, liver) most common
Cure rate: lower vs general population
ATM deficiency fatality: 72%
Overall prognosis: poor compared to non-IEI cancers.
Systematic Review and Meta-Analysis. J Clin Immunol 45, 34 (2025). doi.org/10.1007/s10875…@oncodaily@NatImmunol@CImmunobiology@ESMO_Open
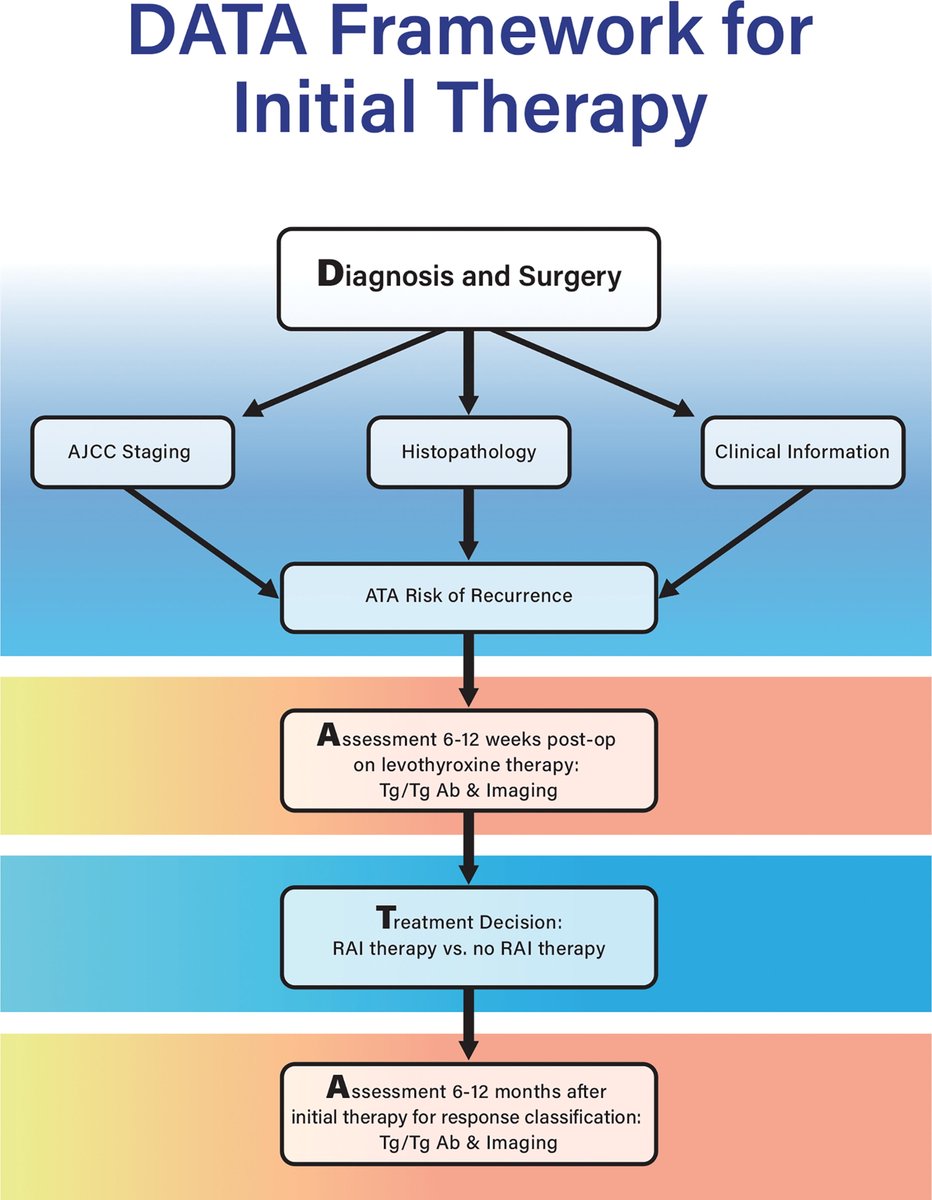
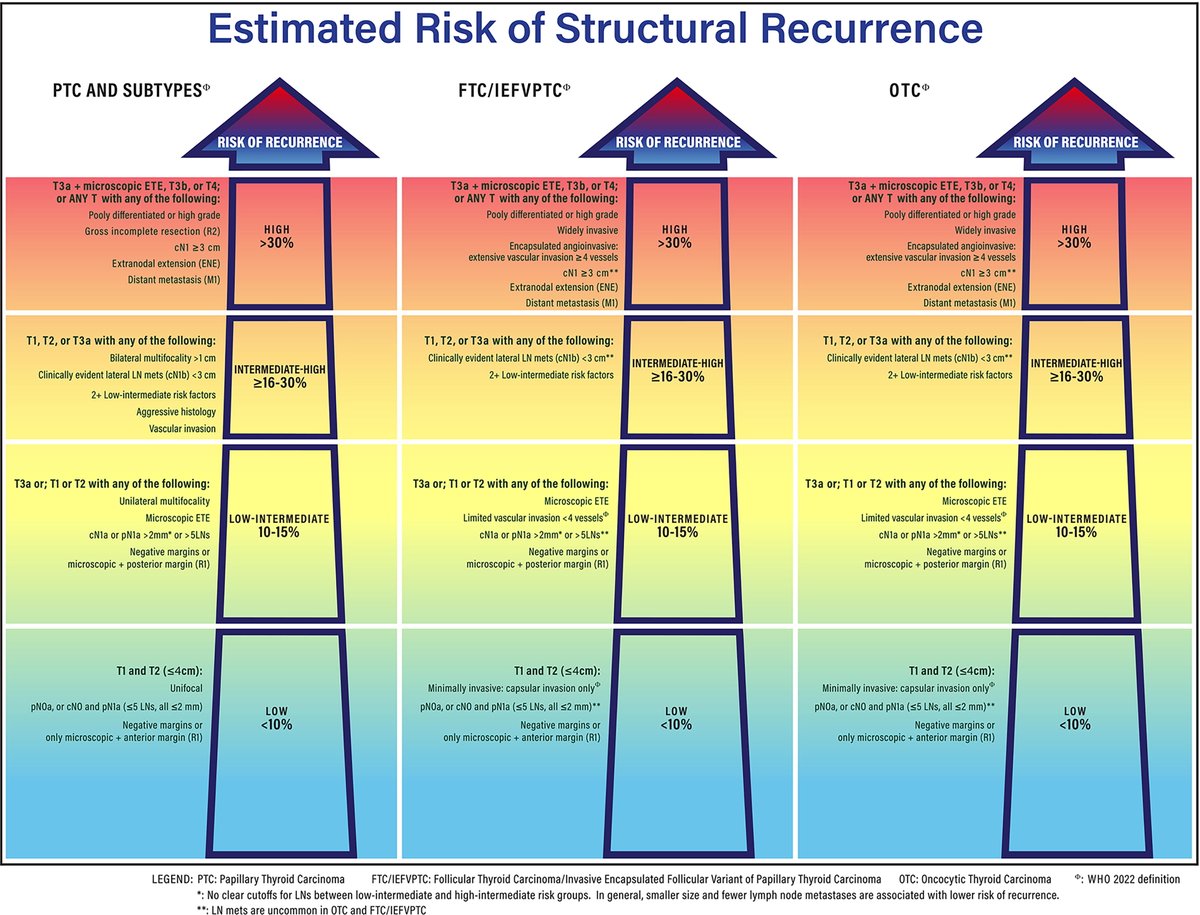
🚨 The 2025 ATA Guidelines for Differentiated Thyroid Cancer mark the first major update in a decade, emphasizing:
🔹 Active surveillance for low-risk patients
🔹 Less aggressive surgery
🔹 Smarter, individualized follow-up
📖 Read more: liebertpub.com/doi/10.1177/10…
“New HER2 ADC Shows Promise Beyond T-DM1 — But Can It Match T-DXd?”
🚨 HER2+ mBC Update
📊 Phase 3 (N=224, China)
🔹 Trastuzumab Pamirtecan (BNT323/DB-1303) vs T-DM1
✅ Significant PFS benefit → primary endpoint met
❓ Why vs T-DM1, not T-DXd?
👉 Trial designed when T-DM1 was global 2L standard
👉 Regulatory path in China still required T-DM1 comparator
🌍 Next: HR+ mBC (DYNASTY-Breast02)
✨ New HER2 ADC contender, but true test will be vs T-DXd
#Oncology#BreastCancer#ADC@Annals_Oncology@myESMO@BreastCancerNow@ASCO@oncodaily
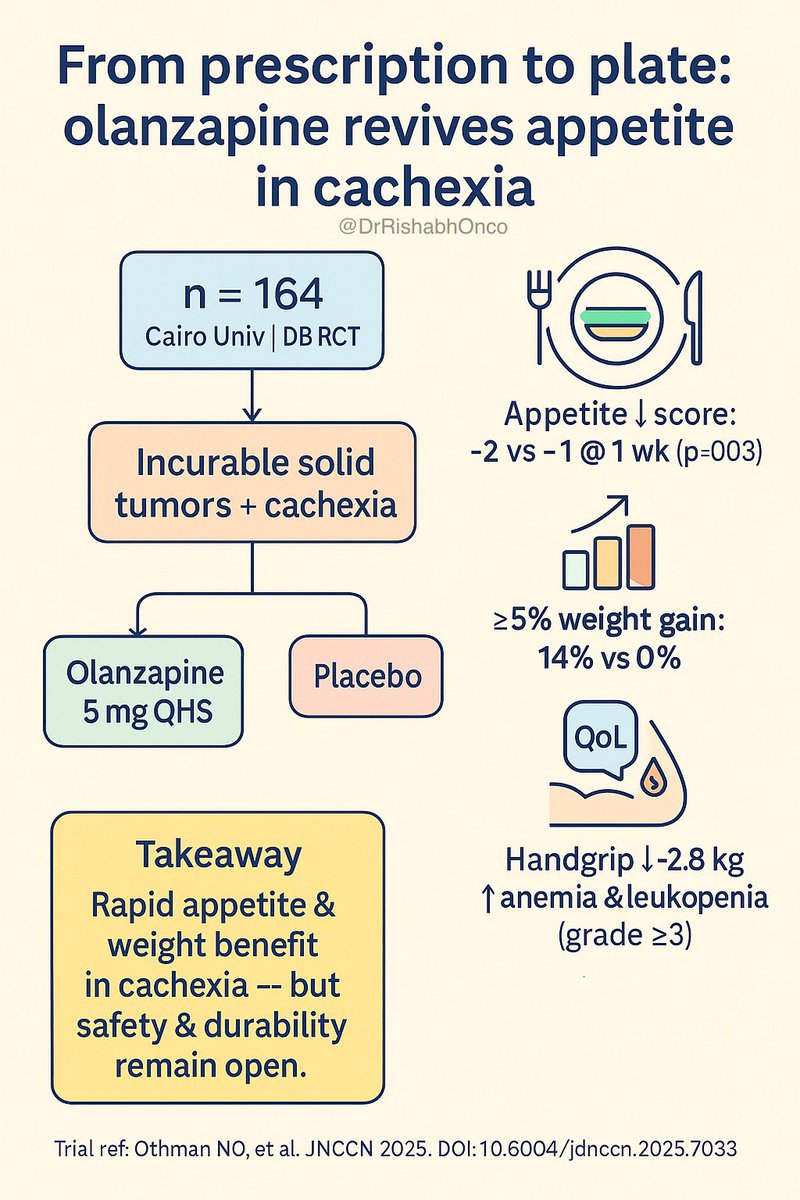
The OlAnCa trial suggests that short-course olanzapine can improve appetite in advanced cancer, but several pitfalls limit its interpretation. The study enrolled a mixed solid-tumor cohort without stratification by cancer type or chemosensitivity, so it remains unclear which tumors truly benefit; improvements may simply reflect disease response in chemosensitive cancers, since concurrent palliative therapy was allowed but not rigorously analyzed. Cachexia is a chronic process evolving over months, yet follow-up was only 4 weeks, too short to meaningfully assess body composition or functional outcomes. Results rely heavily on a single subjective ESAS item, showed discordance with ACS at 4 weeks, and were confounded by high attrition and per-protocol shrinkage. The trial was single-center (Egypt), raising concerns about generalizability, and safety signals (anemia, leukopenia, hyperglycemia, CNS effects) were more frequent than in prior antiemetic studies. Finally, there was no active comparator (e.g., megestrol or steroids), making it difficult to position olanzapine against current standards. Overall, the trial provides an important signal for rapid short-term appetite benefit, but questions remain about durability, cancer-specific benefit, and real-world applicability.