Sunil Solar MD
1.2K posts

Sunil Solar MD
@CardioDocDexter
DM Cardiology (AIIMS, New Delhi) | Profound #Cricket 🏏 Fanatic #Medtwitter
India🇮🇳 Katılım Ocak 2021
825 Takip Edilen1.8K Takipçiler

Six months old child presented with central cyanosis and echocardiography was suggestive of DORV VSD and PS .
Color doppler at IVS is suggestive of swiss cheese VSDs.
English
Sunil Solar MD retweetledi
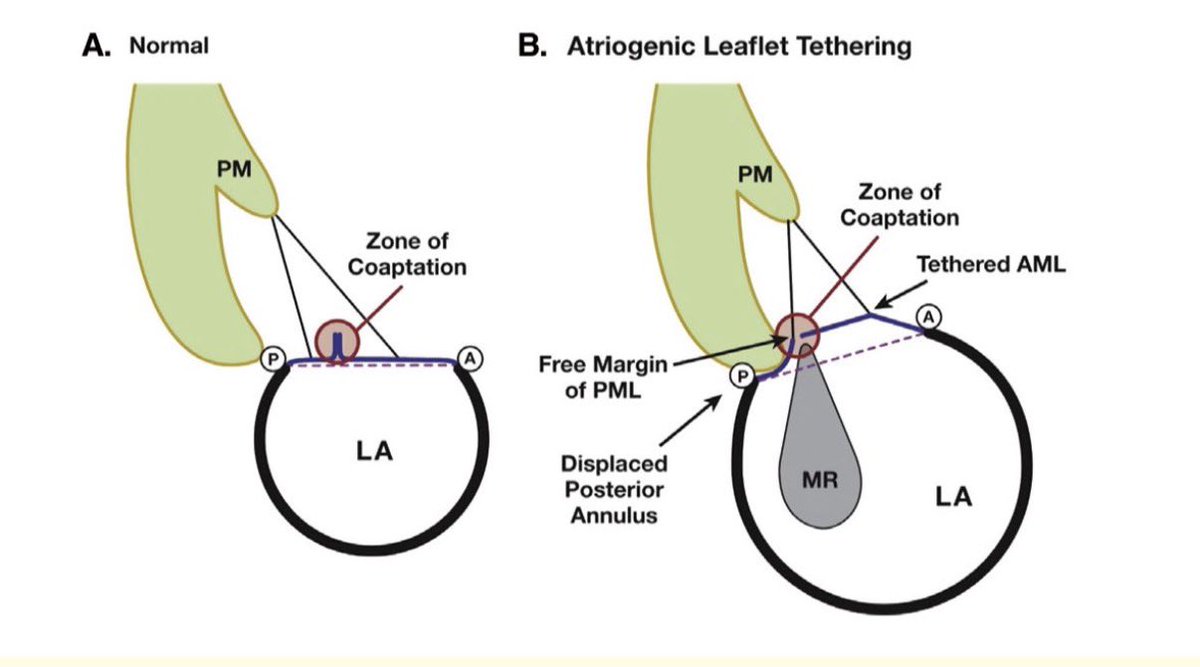
42-year-old lady with recurrent palpitation, exertional chest pain and fatigue. What could be the mechanism of severe mitral regurgitation ?
English
Sunil Solar MD retweetledi
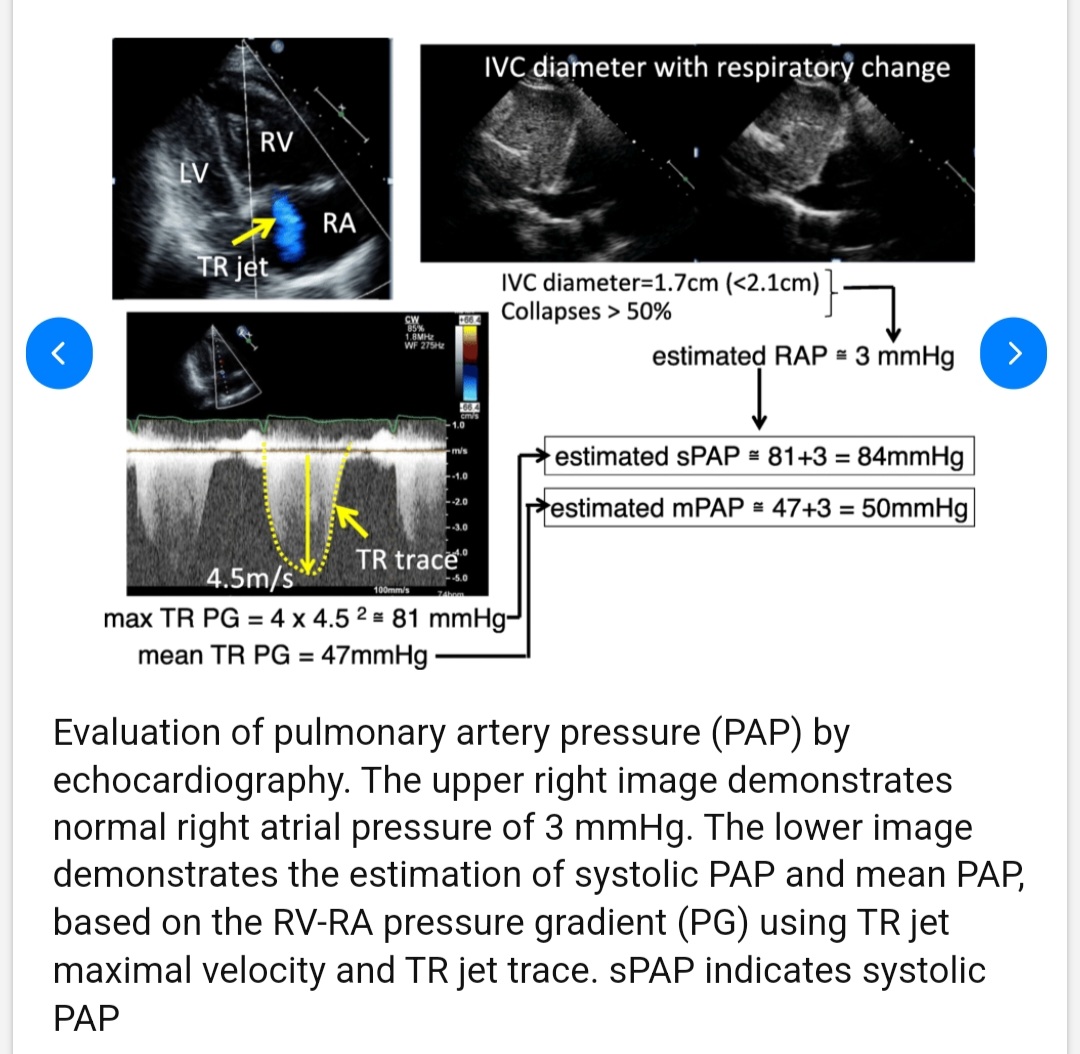
40-year-old gentleman with uncontrolled systemic hypertension, what are the DTA CW doppler findings ?

English
Sunil Solar MD retweetledi

🧬 LMNA cardiomyopathy: not all patients progress the same.
Now we can quantify who will.
We’ve become good at predicting:
👉 sudden death
👉 arrhythmic risk
But heart failure?
👉 Still a blind spot in laminopathies
💥 This paper changes that.
For the first time:
👉 a dedicated risk model for HF progression in LMNA patients
📊 The reality (and it’s not reassuring):
• HF-MACE in ~10% at 5 years
• ~45% lifetime risk by age 70
And if LVEF <30%:
👉 50% events within 1 year
ehag104
⚡ Four variables. That’s it.
Independent predictors of HF progression:
• Male sex
• LVEF <50%
• Missense variants (head/rod domains)
• Complete LBBB
🔥 Translation:
👉 Genetics + conduction + early LV dysfunction
= the HF trajectory is already written
📉 What’s really striking (Figure 4):
• 0 risk factors → ~1.5% at 5 years
• 1 factor → ~5%
• ≥2 factors → ~22%
➡️ Not a spectrum
➡️ A stepwise risk escalation
🧠 And here’s the key insight:
👉 Even with preserved EF, risk is not low
Patients with LVEF ≥50% + risk factors:
→ still meaningful HF risk (~11% at 5 years)
ehag104
⚠️ This challenges our mindset:
We wait for EF to drop
👉 But the disease is already progressing
💡 Clinical implication (this is the real shift):
Risk stratification in LMNA should not be:
❌ reactive
❌ EF-driven
But:
👉 proactive + genotype-informed
🚀 What this enables:
• Earlier follow-up intensification
• Earlier HF therapy
• Earlier referral for advanced HF pathways
• Better selection for trials
🎯 Take-home message
LMNA cardiomyopathy is predictable.
👉 Not just arrhythmias
👉 Heart failure too
And if we wait for severe dysfunction…
👉 we are already late
💬 Should we start treating LMNA patients before EF declines?
#Cardiology #LMNA #Cardiomyopathy
#HeartFailure #Genetics
#PrecisionMedicine #EPeeps #CardioTwitter 🧬🫀
doi.org/10.1093/eurhea…

English
Sunil Solar MD retweetledi

Cardiologists in India are invited to apply for the ACC's 🆕 Cleveland Clinic Global Scholar Award, offering a three- to four-week observership at Cleveland Clinic & recognition at #ACC27-#WCCardio in Houston, TX.
Learn more & submit by June 8 ➡️ bit.ly/41Ig7aR #ACCAsia

English
Sunil Solar MD retweetledi

Out of 72 definitions, the JACC CV expert panel definition of atrial functional MR was strongly associated with outcomes. @JACCJournals
What are the differences in the Atrial Functional MR definition (ESC vs JACC)?
🫀 1. Left Atrial Size Threshold (LAVI)
-> ESC Definition (More Inclusive / Earlier Stage, Threshold: LAVI > 34 mL/m²
->JACC Definition (More Restrictive / Clinically Advanced)
Threshold: LAVI ≥ 40 mL/m²
🍃 2. Leaflet Motion Criteria (Carpentier Classification)
-> ESC: Only Type I (Normal Motion)
Mechanism: Pure annular dilation
-> JACC: Type I
Mild Type IIIb (posterior leaflet restriction)
Mechanism: Annular dilation + tethering
("Extreme LA enlargement draws the posterior annulus toward the epicardial surface, increasing the annulo-papillary distance".)
Papers:
sciencedirect.com/science/articl…
@WilliamZoghbi
#ACCImaging #CVimaging #Echofirst

WilliamZoghbi@WilliamZoghbi
Hot off the press! My Editorial in JACC on Atrial functional MR. Among 72 definitions of AfMR (!!) in the literature, Koschatko et al demonstrated that the one provided by JACC CV Imaging Expert Panel in 2022 was the most powerful in predicting outcome. pubmed.ncbi.nlm.nih.gov/41949521/
English
Sunil Solar MD retweetledi
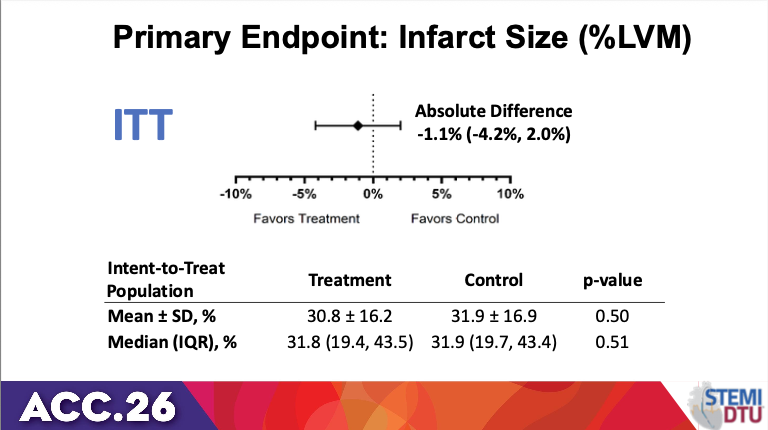
#STEMI DTU # ACC26
Mechanical Circulatory Support Doesn’t Reduce Infarct Size in STEMI
❤️“Time is myocardium” - this trial challenged that
⏱️ Deliberately delaying PCI to unload the LV first
🩸 Impella support— ~6x more bleeding/vascular complications
🤯 Delaying PCI by ~45 min didn’t worsen infarct size—but also didn’t meaningfully help it either
💫Impella is good for cardiogenic shock—not for routine STEMI strategy based on #STEMIDTU
@mmamas1973 @mirvatalasnag @SrihariNaiduMD



English
Sunil Solar MD retweetledi

🫀Heart failure in 2026: we are no longer treating symptoms. We are redesigning the disease.
The latest evidence update reminds us of something profound:
Heart failure is no longer a single entity.
It is a spectrum, and now, finally, we are treating it as one.
Several paradigm shifts stand out.
1. SGLT2 inhibitors are no longer “add-on” therapy.
They are foundational across the entire EF spectrum.
From HFrEF to HFpEF, the data are now consistent.
Not just symptom improvement, but hard outcomes.
This may be the most important unifying therapy in modern HF.
2. HFpEF is no longer a therapeutic desert.
For the first time, we have real disease-modifying options:
Finerenone → outcome reduction across EF ranges
GLP-1 / dual incretin therapies → targeting the obesity phenotype
Structural and metabolic mechanisms are finally being addressed
We are moving from “HFpEF frustration” → HFpEF phenotyping.
3. Acute heart failure is no longer about stabilization.
It is about early transformation.
The new paradigm:
Start GDMT in-hospital
Optimize rapidly
Treat beyond congestion
Decongestion is still important, but it is no longer the goal.
Disease modification starts on day 1.
4. Decongestion is becoming precision medicine
Urine sodium-guided therapy
Early escalation of loop diuretics
Sequential nephron blockade
Not just “give furosemide”, but measure, adjust, and target response.
5. Devices are no longer rescue therapy, they are integrated care
TEER expanding from mitral → tricuspid
Pulmonary artery pressure monitoring reducing hospitalizations
Remote hemodynamics shaping outpatient management
The boundary between ICU, ward, and home is dissolving.
6. The biggest problem is no longer evidence.
It is implementation.
We already have:
Quadruple therapy
Proven outcome benefits
Yet many patients never reach target doses.
The gap is no longer science.
It is execution.
🤓Final message
Heart failure care has entered a new era:
Mechanism-based therapy
Early aggressive optimization
Phenotype-driven treatment
And perhaps most importantly:
We are no longer chasing symptoms.
We are altering the trajectory of the disease.
📃Reference
Liori S, et al. Heart failure evidence update 2026. Heart Failure Reviews. 2026. doi.org/10.1007/s10741…

English
Sunil Solar MD retweetledi
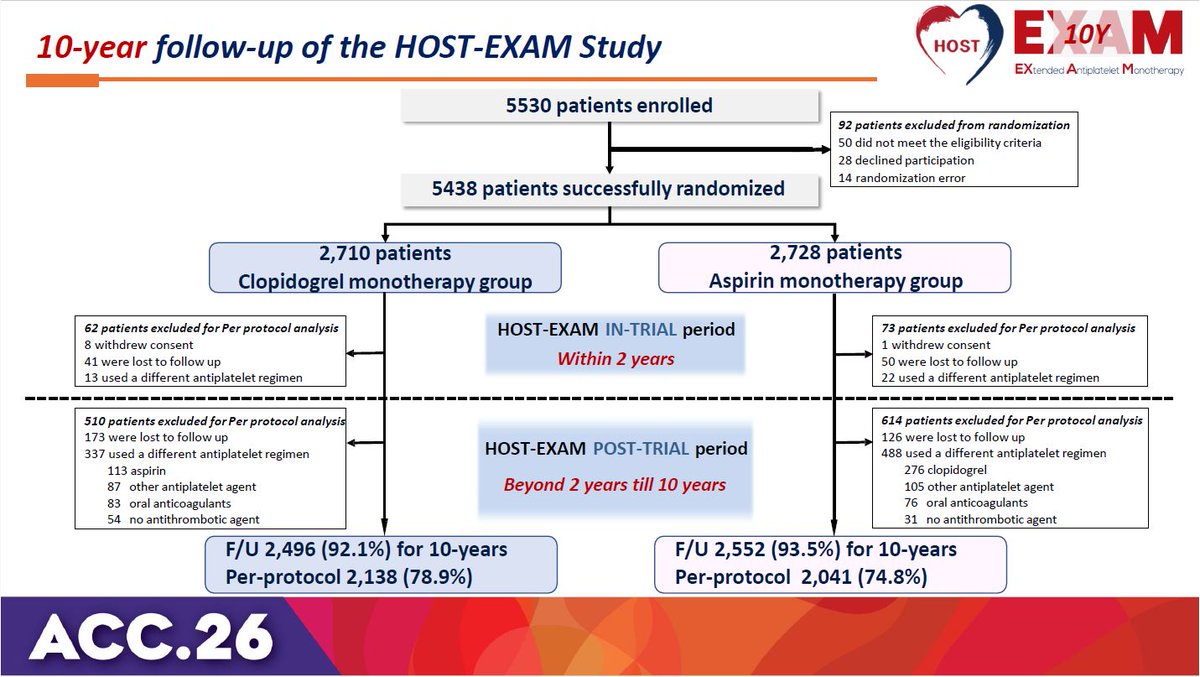
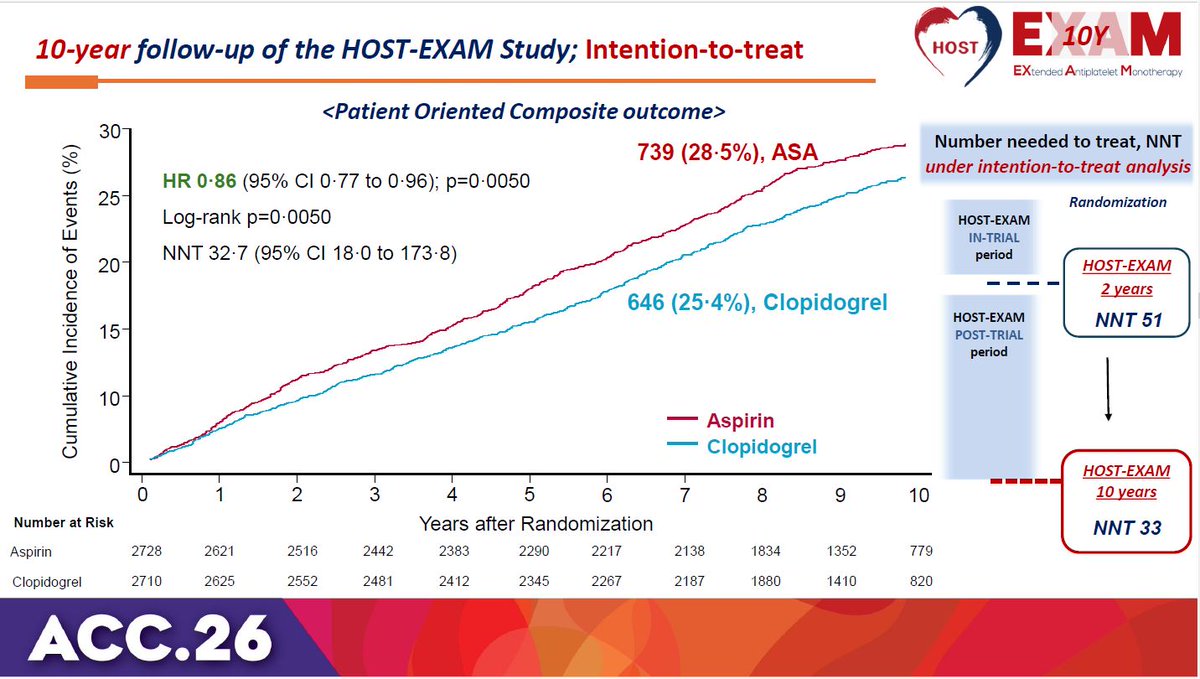
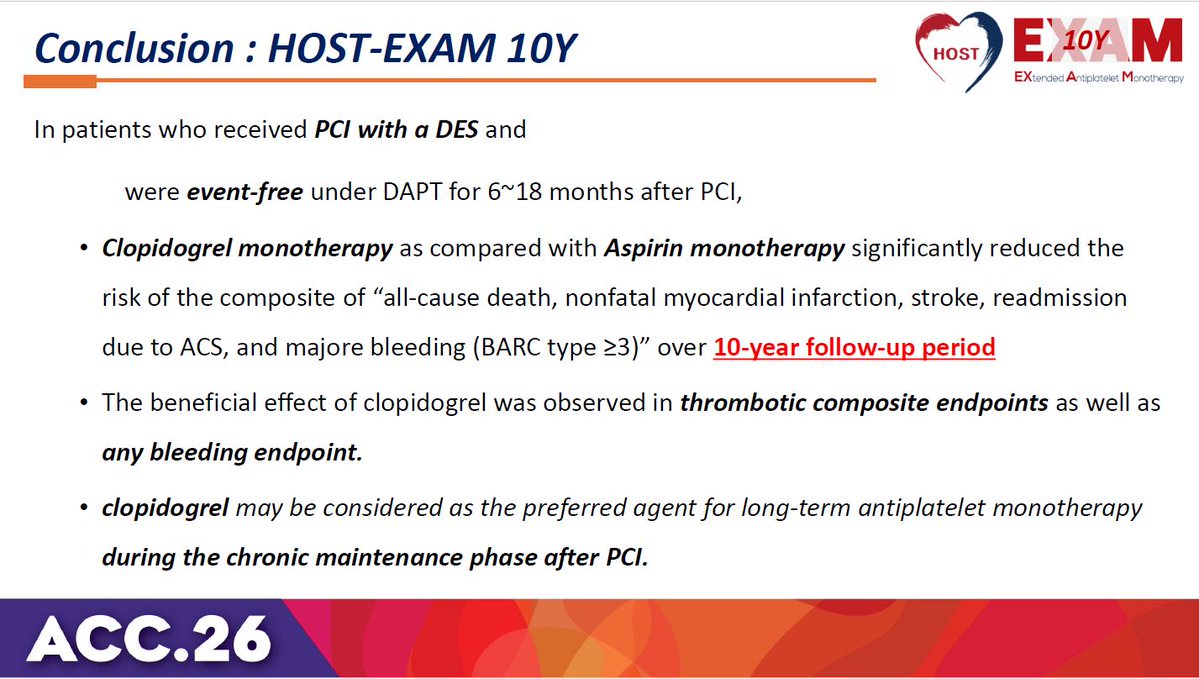
HOST-EXAM trial 10-year results: Clopidogrel monotherapy is superior to aspirin for chronic maintenance after PCI, significantly reducing both thrombotic and bleeding events. #ACC26 View slides here: clinicaltrialresults.org/wp-content/upl…

English
Sunil Solar MD retweetledi

1/16 🧵 ORBITA-CTO: The first randomized, placebo-controlled trial of CTO PCI.
📰 Published in JACC, presented at #ACC26.
🔬 Finally, sham-controlled evidence for what we do in the cath lab every day.
One of the best designed studies I have ever seen!
A biostatistical deep dive. Let's go. 👇
English
Sunil Solar MD retweetledi

“Hamstring leaflet” or Atriogenic leaflet tethering secondary to AF induced atrial remodelling may be confused with RHD as PML tethering is a feature of rheumatic process. At least a few answered it as RHD. Thanks to @iamritu for highlighting this first through X and I learned about hamstring leaflet in Atrial secondary MR from Dr Ritu.
English
Sunil Solar MD retweetledi

With rising cancer incidences in India, finances play a huge impact in care. A brief guide on Govt. schemes to help patients in their time of need.
1. Ayushman Bharat (PM-JAY) -good for basic treatment but 5 lacs pa is insufficient and majority advanced treatments not covered
English
Sunil Solar MD retweetledi
This is the fastest way to break someone down
English
Sunil Solar MD retweetledi

Cardiogenic Shock: @NEJM
🥸 A contemporary perspective on cardiogenic shock by @thiele_holger
😱 Outstanding - here is a summary
👇👇👇

English
Sunil Solar MD retweetledi

President Trump is taking 325 mg of aspirin a day to prevent heart disease. His doctors advise him to take 81 mg. Both are wrong. Here’s why.
New edition of Ground Truths, open-access
erictopol.substack.com/p/the-lowdown-…

English
Sunil Solar MD retweetledi

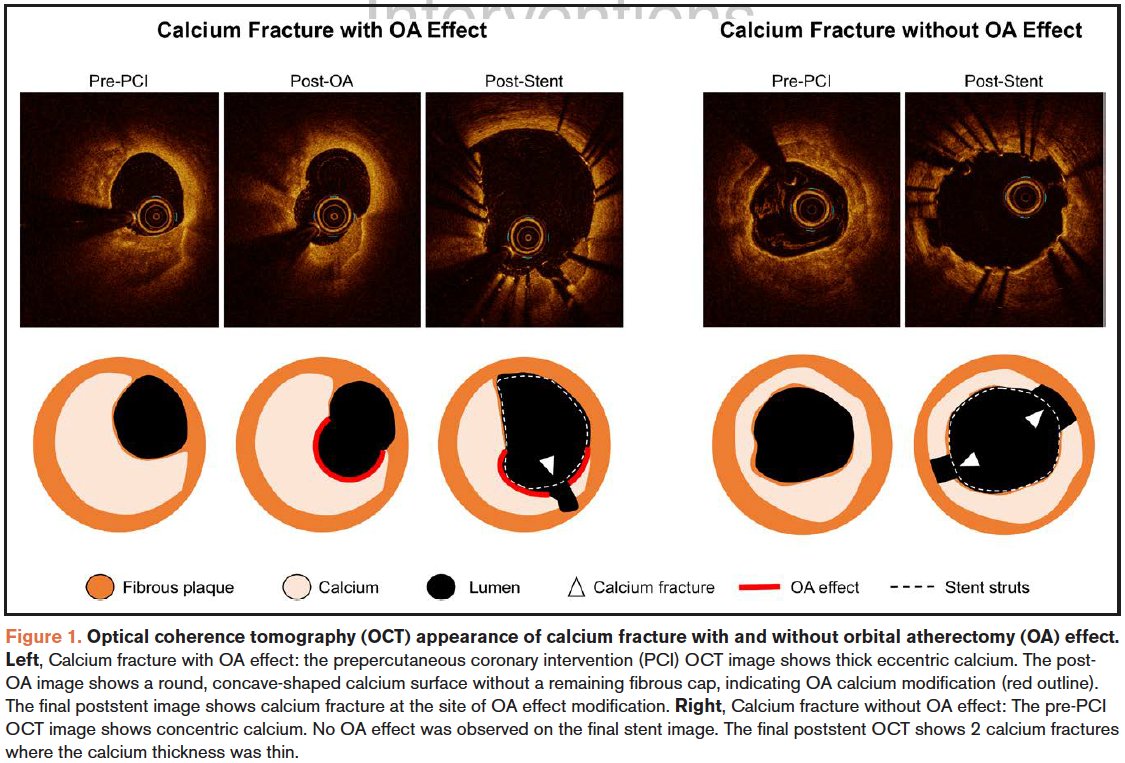
Our core lab OCT substudy from ECLIPSE now publ in Circ CV Int. Although 98.1% of 578 lsns were severely calcified by angio, <half met OCT criteria for severe calc (arc ≥270°). Min stent area was not larger w/atherectomy vs balloon pre-dil, even in severe lsns. Happy new year!🎉

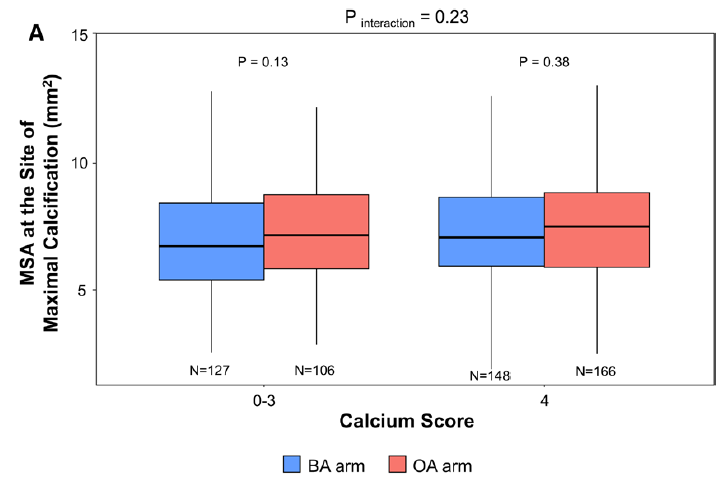
English
Sunil Solar MD retweetledi

This year, 2025, I have published 9 articles on Cardiac Rehabilitation.
My goal is to increase awareness of the importance of Cardiac Rehabilitation for our patients in clinical practice, from its positive impact on mortality to quality of life in different CV conditions!

English
Sunil Solar MD retweetledi
60 mm Biomime Morph tapering stent entering LAD like Vande Bharat express 😁. Make in India💪💪💪
English
Sunil Solar MD retweetledi
Two descending thoracic aortas in parallel?!! Nope. It is a post operative case. Guess the surgery?
English
Sunil Solar MD retweetledi