David Erlinge retweetledi

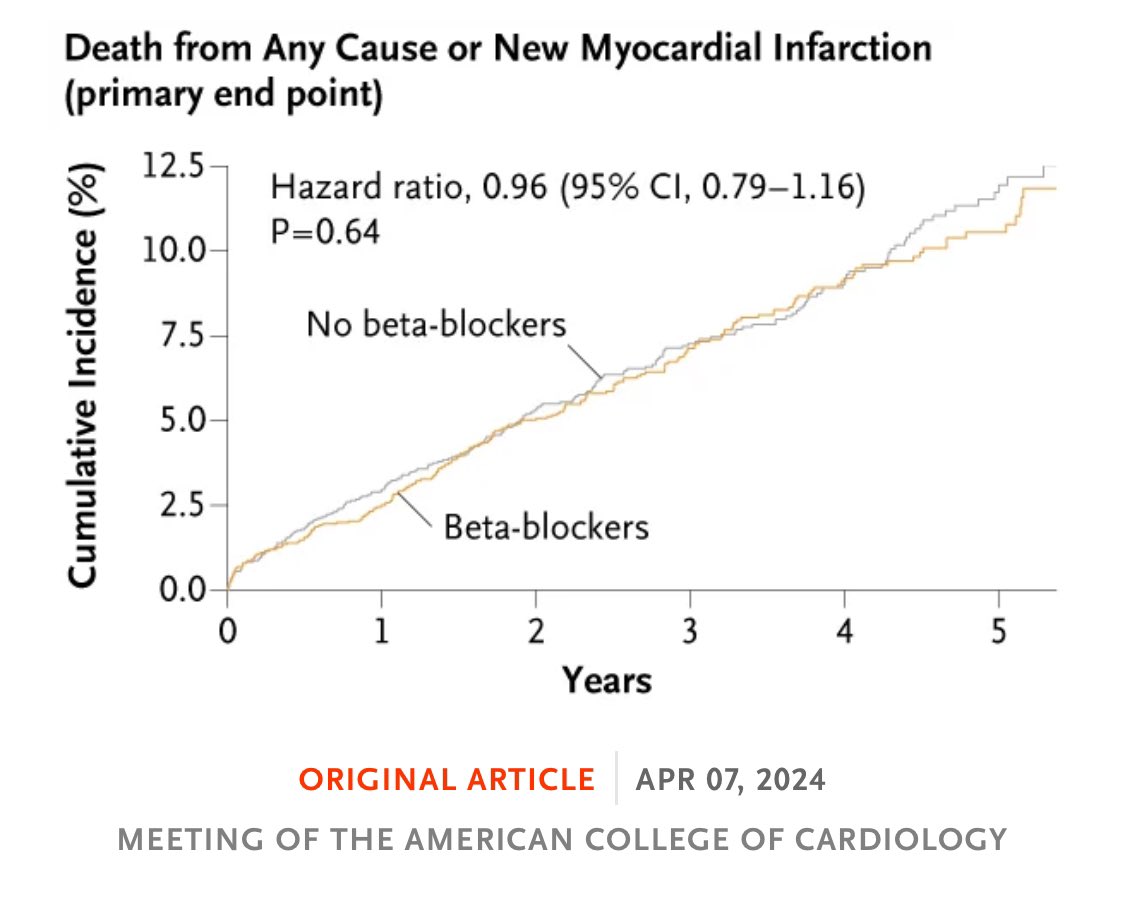
Congratulations to @YndigegnY for a successful defence of his PhD today (1st author of REDUCE-AMI trial doi.org/10.1056/nejmoa… ) at the University of Lund (I was the external examiner) with supervisors @AlexSchiopu10 and @DavidErlinge
This was a public examination with a strong defence. Thankfully Mrs Yndigegn is still inviting me to the evening dinner celebration in honour of her husband 😜
Thank you to David and Alex for hosting me in Lund with a memorable dinner last night



English