
David Rees
1.1K posts

David Rees
@DavidRees1985
ICM & Anaesthesia Consultant. TTE & TOE, Heart/Lung failure, ECMO & Transfer.
London, England Katılım Eylül 2011
1.3K Takip Edilen484 Takipçiler


Richard Whiffin and Scott Sneddon have done an incredible job with the Welsh 20s.
Hat tip, gents. 👌
English
@Hurricane15 @thepaulwilliams The ref was equally terrible reffing both sides. Was consistently awful.
English
@thepaulwilliams The ref did what can only be described as a HIDEOUS job which if allowed will ruin our sport.
English
David Rees retweetledi

Applications are now open for ACCESS Consultant posts. We’re hiring NHS Consultants in Critical Care or Anaesthesia to join the service. This is a flexible, fixed-term opportunity offering 1-4 PAs. Any interests or questions get in touch with the team. jobs.nhs.uk/candidate/joba…

English
David Rees retweetledi
Another milestone reached! 🎉 3000 completed transfers! 🚀 Huge thank you to everyone for making this happen! @NHSBartsHealth @imperialcollege @GSTT_ICU @GivingtoGeorges @Ldn_Ambulance @NHSEnglandLDN @drmamoun01 @LucyJ1982 @iancarbar @DoctorAmbroise @DrSanjChana @DavidRees1985
English

English
David Rees retweetledi
🚨 We're hiring! Seeking NHS Consultants in Critical Care Medicine or Anaesthesia for London's Adult Critical Care Emergency Service (ACCESS). Fixed-term, flexible 1-4 PAs. Make a difference in critical care & get in touch with the team. bartshealth.nhs.uk/jobs#!/job/-v6…. #NHSJobs #ACCTs

English
David Rees retweetledi
🚀 3,000 Referrals in just 16 months post-launch! Thank you to everyone who made this possible. Special thanks to our Senior Leadership Team who continue to drive our mission. @drmamoun01 @LucyJ1982 @iancarbar @DoctorAmbroise @DrSanjChana @DavidRees1985 @Ldn_Ambulance
English
David Rees retweetledi

What great way to finish the summer Bart’s ECMO Course . Fantastic MDT learning and immersive simulation.
Few spots left for the September course .
@GomorraDoc @sachindoc @Caroline_gasdoc @drmamoun01 @Novicelearner9 @itariq14




English

@doctimcook @ShaunLintern @NHSBartsHealth 2 very contrasting and sad cases. I think overwhelming majority would consider heavily tranquillizing a critically unwell patient would be incredibly risky and not sensible. The 2nd case would split opinion. The conclusions made from that case many would disagree with.
English

It’s interesting that this case
- which rests with the decision to sedate rather than anaesthetise (which is judged here to be safer)
judiciary.uk/prevention-of-…
Comes in the same week as this case
-in which the criticism is of the decision to undertake general anaesthesia instead of deep sedation
(which is judged here to be safer)
judiciary.uk/prevention-of-…
Both key to recommendations to prevent future deaths
Albeit both may be right….
….medicine is complex and requires careful, often time sensitive, high stakes decisions and actions. Anyone telling you otherwise doesn’t understand and hasn’t done it.
English

A 38-year-old black man died at @NHSBartsHealth after a flawed decision to sedate him. Coroner criticises "coping culture" and the trust response including governance failures and poor effort by lawyers #patientsafety


English
@lzavorszky @armycritcare Pretty sure the norad and angio in a frail end stage dementia patient would also fall into the "not altering the ultimate outcome" bracket too.
English

@armycritcare That was the resolution of this case.
Perc patch closure was considered but deemed technically difficult and not altering the ultimate outcome.
English
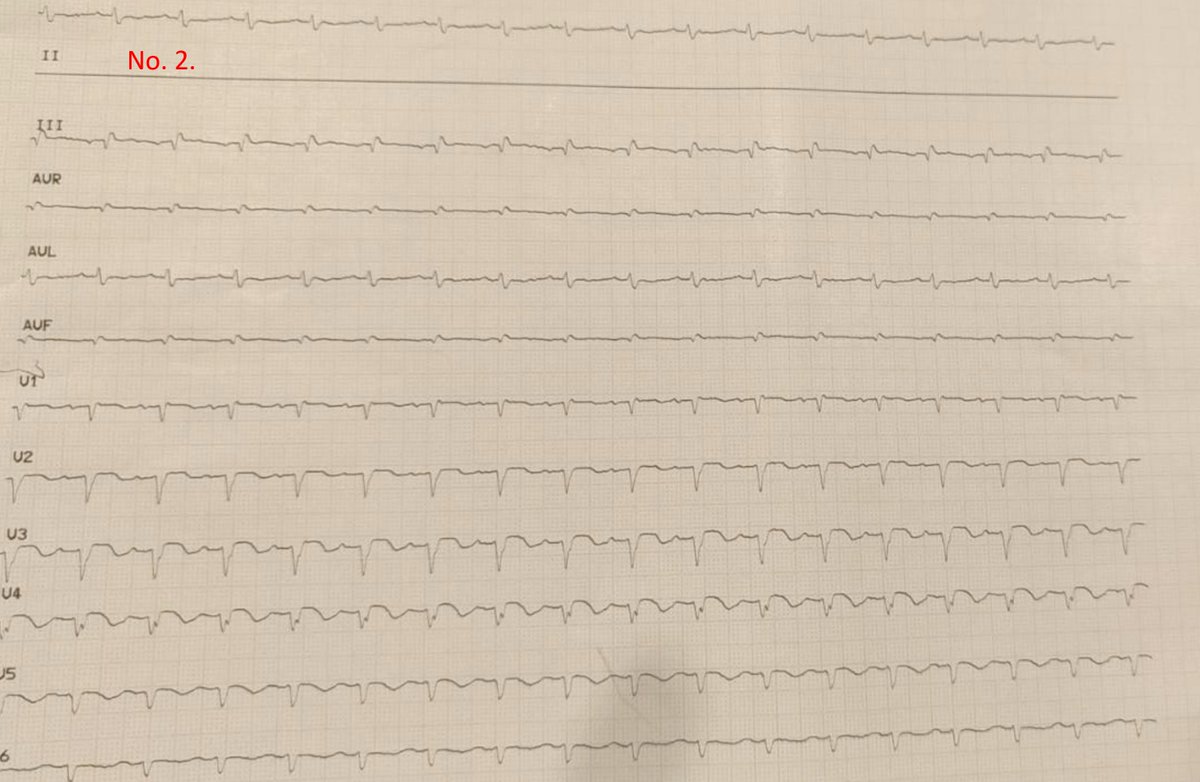
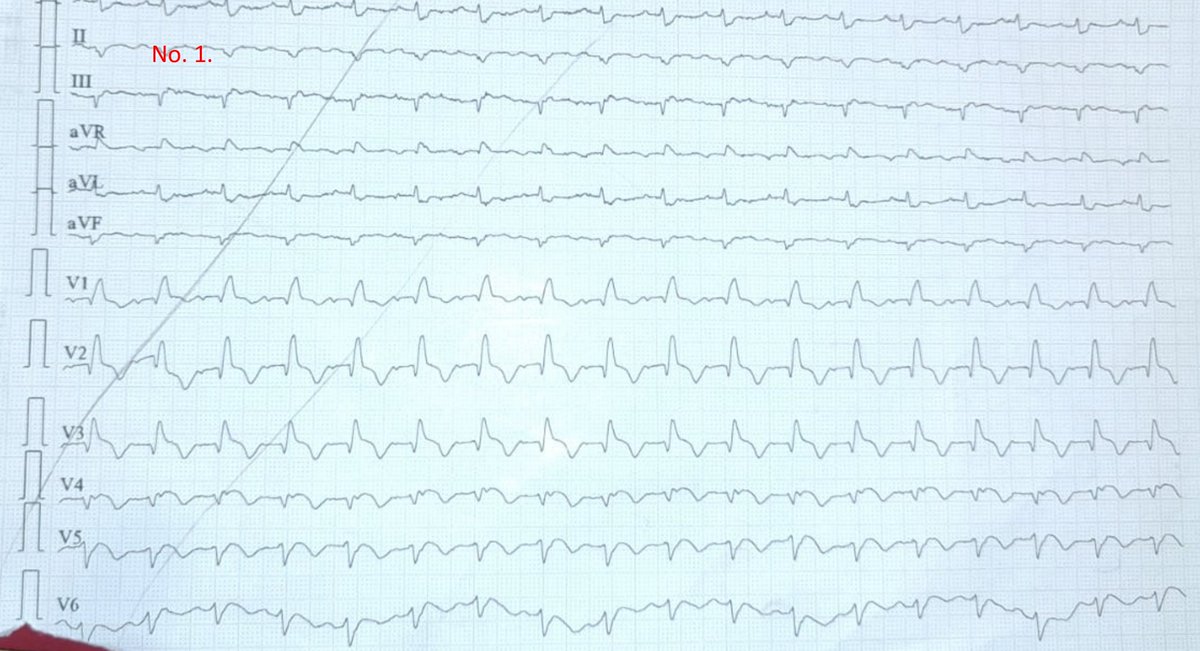
71 y/o old reffered to PCI centre
Not responding to calls (known living w/ severe dementia, carers). 🚑 to small ER.
A&B maintained but high metabolic acidosis and hypotensive on 0.3 ug/kg/min norepi. High Trops.
Admission and +6hr ECG, Echo by untrained ED doc. Next step?
GIF
English
@PBSherren In potentially a "normal" or small LV cavity size like in that example would it push you towards / away from specific vent strategies? E.g Issue of suction events in that scenario with ECPELLA?
English

LV venting discussion needs more nuance beyond LVEDP alone. With high ECBFs/good bicaval access there's limited transpulmonary blood flow/LVEDP issues but if no ejection and intracardiac stasis, may still be 'vent' need to avoid intracardiac clot even if non-distended/low LVEDP
English
David Rees retweetledi
🎉Celebrating one year since the launch of ACCESS! 🚀 Huge thanks to our amazing staff, colleagues, stakeholders, and units across London for their incredible support and dedication. Here's to many more milestones !
English
@drp297 @iceman_ex @jdrwilcox @VirtueOfNothing @AjEusuf @TRICNetwork @echonepean @chrisfduncan @jsemccm @GSTTnhs @UHWCriticalCare Many examples of exactly this around 🇬🇧. In fact some of the best POCUS / Echo clinicians in the UK, and FUSIC leads, aren't tertiary or cardiac based, delivering such models. 3/.
English

@DavidRees1985 @iceman_ex @jdrwilcox @VirtueOfNothing @AjEusuf @TRICNetwork @echonepean @chrisfduncan @jsemccm @GSTTnhs @UHWCriticalCare I would argue a physiologist is cheaper than a consultant..... And the opportunity cost, significantly more important.
For smaller places, I would imagine a physiologist to do all inpatient scans, but with a focus on ITU might work as a concept? With a flexible workload
English

This classic paper by @susannaprice on levels of training in intensive care echocardiography from 2008 remains incredibly relevant
#echofirst
ncbi.nlm.nih.gov/pmc/articles/P…
English
@drp297 @iceman_ex @jdrwilcox @VirtueOfNothing @AjEusuf @TRICNetwork @echonepean @chrisfduncan @jsemccm @GSTTnhs @UHWCriticalCare Hence to justify the WTE you need the volume of requests. The secondary benefit to improved service delivery / governance is the education and everyone wins. In lower workload areas, part time input isn't a dedicated service. This then needs delivery from within. 2/.
English
@drp297 @iceman_ex @jdrwilcox @VirtueOfNothing @AjEusuf @TRICNetwork @echonepean @chrisfduncan @jsemccm @GSTTnhs @UHWCriticalCare From experience in recruitment I would say the reality is the opposite. Physiologists in short supply with large workload already. For dedicated service you need 1 WTE at 8A (vs approx 4 DCC's) for consultant. Most consultants are delivering within job plan also. 1/2.
English
@iceman_ex @jdrwilcox @drp297 @VirtueOfNothing @AjEusuf @TRICNetwork @echonepean @chrisfduncan @jsemccm @GSTTnhs @UHWCriticalCare But you have to have high volume scan requirement to justify the physiologist job plan and cost. Big centre esp cardiac, no problem. Smaller unit however much harder to finance and ultimately need critical mass of intensivists to deliver. 2/2.
English
@iceman_ex @jdrwilcox @drp297 @VirtueOfNothing @AjEusuf @TRICNetwork @echonepean @chrisfduncan @jsemccm @GSTTnhs The 🐘 in the room is money. The ICU physiologist works well if fully integrated and learns the ACCE component and its use on ICU. @UHWCriticalCare has this and it works really well. Excellent governance, access to scans and education for everyone. 1/2.
English
@Manoj_Wickram @iceman_ex @cianmcdermott @emma_bowcock @nat_echo @MaxRidley3 @SmallzAlex Yes. Used in pre vs post capillary Pulmonary HTN differentiation. Instigation of pulm vasodilating therapy Vs offloading and optimizing LV relaxation / flow. Paired with RV function and RV-PA coupling assessment.
English

Is anyone using pulmonary acceleration time as a data point in differentiating between pre and post capillary pHTN? Interested to know your thoughts @iceman_ex @cianmcdermott @emma_bowcock @nat_echo @MaxRidley3 @SmallzAlex
English
@Resuspiece Yes but with the caveat that as it's mandatory it should be fully funded and provided for all those on the resus teams.
English

If you’re part of the crash team, should you have a valid ALS certificate?
English