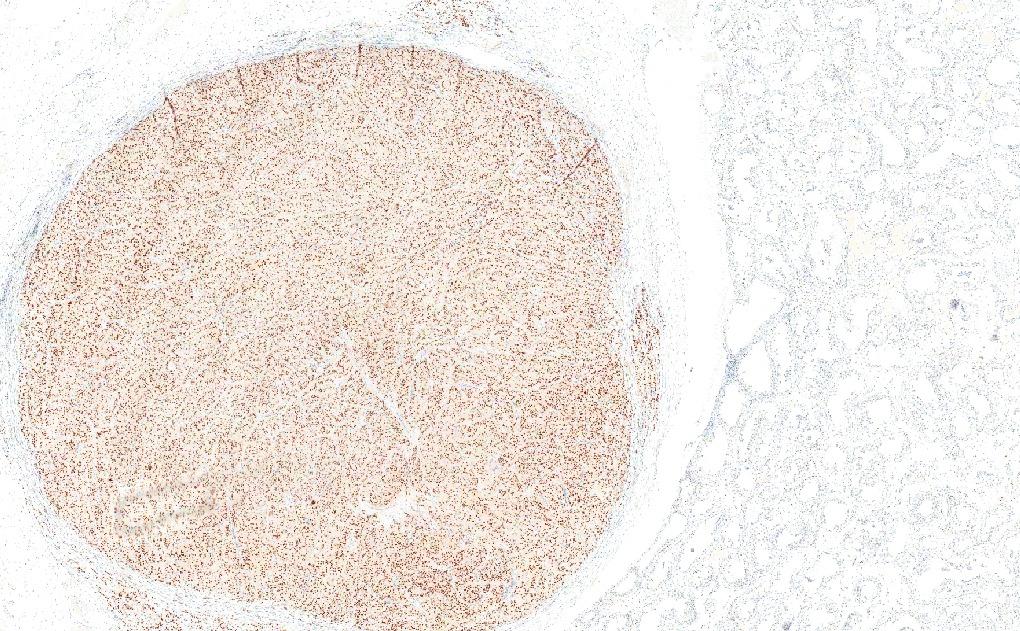
Neuroendocrine tumors of the breast
WHO 6th edition (beta version online)
1. Primary neuroendocrine tumors (grade 1 or 2)
2. Primary neuroendocrine carcinomas: Small cell NEC is only recognized.
***Large cell neuroendocrine carcinoma is no longer recognized as a separate breast entity and should be reclasified as IBC NST with neuroendocrine differentiation***
Dr. Tan #USCAP2026#pathology#PathX#PathTwitter#everydaybreastpath
✅ Leydig Cell Tumor 🎯🔬
• Polygonal cells with abundant eosinophilic to lipid-rich cytoplasm and prominent nucleoli
• Often produces estrogens leading to gynecomastia; Reinke crystals are pathognomonic
• Malignant cases frequently harbor MDM2 and CDK4 amplifications
• MDM2 amplification drives aggressive behavior and can be detected by IHC
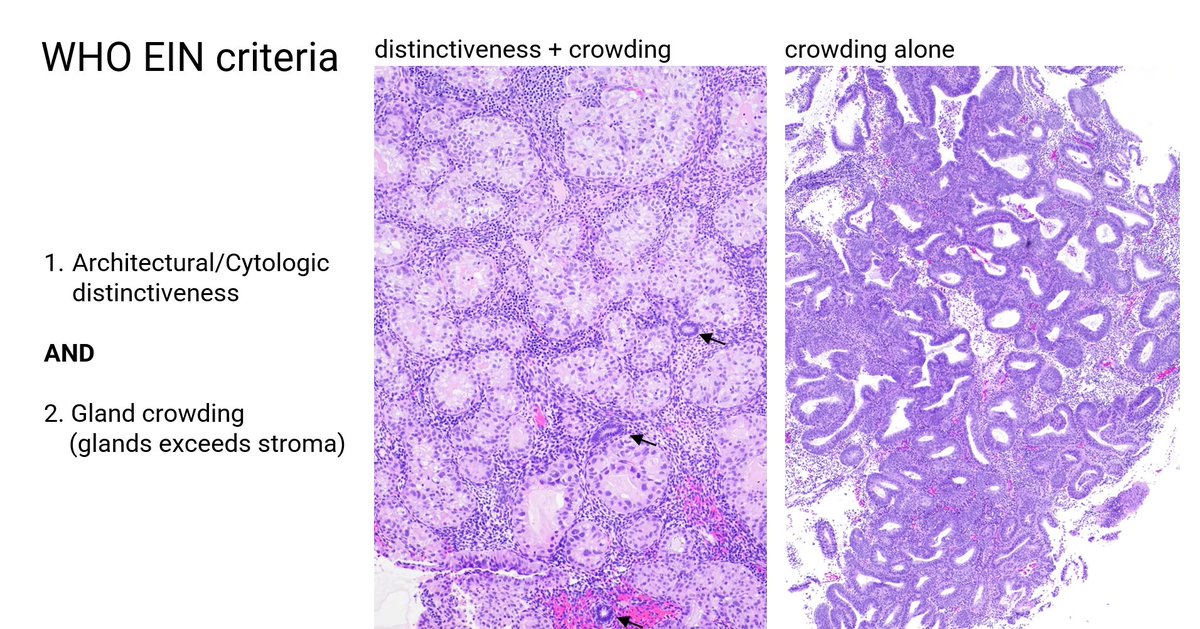
WHO endometrioid intraepithelial neoplasia/atypical hyperplasia (EIN/AH) criteria
1. Architectural/cytologic distinctiveness
AND
2. Gland crowding (glands exceed stroma)
Case on the left: Meets criteria 1 and 2.
Case on the right: Crowding alone. What should you do? EIN/AH diagnosis can fit in this case
***The diagnosis of EIN sometimes requires a flexible approach.***
Dr. Castrillon #USCAP2026#pathology#PathX#PathTwitter#everydayGYN
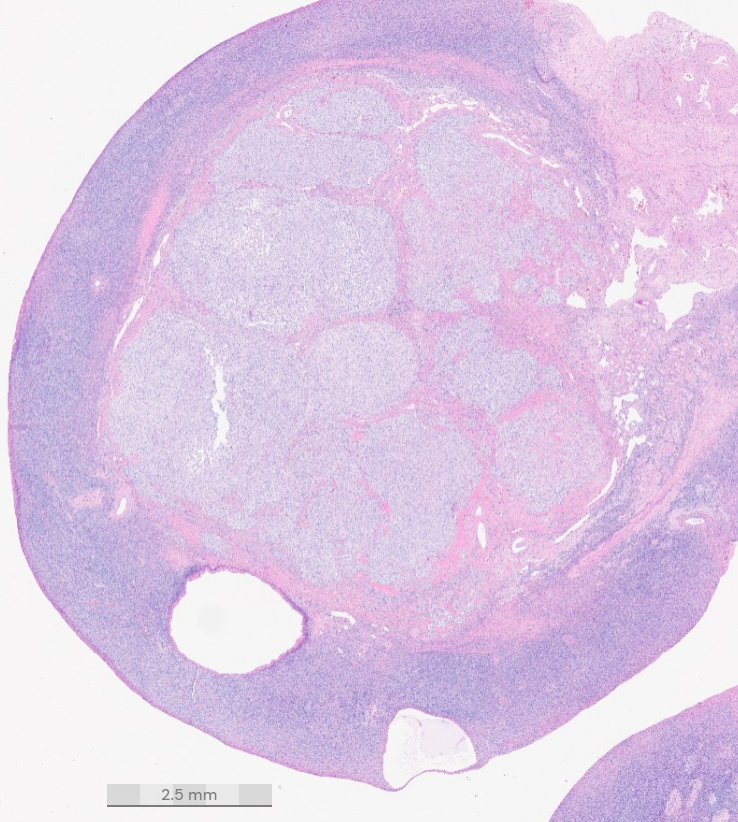
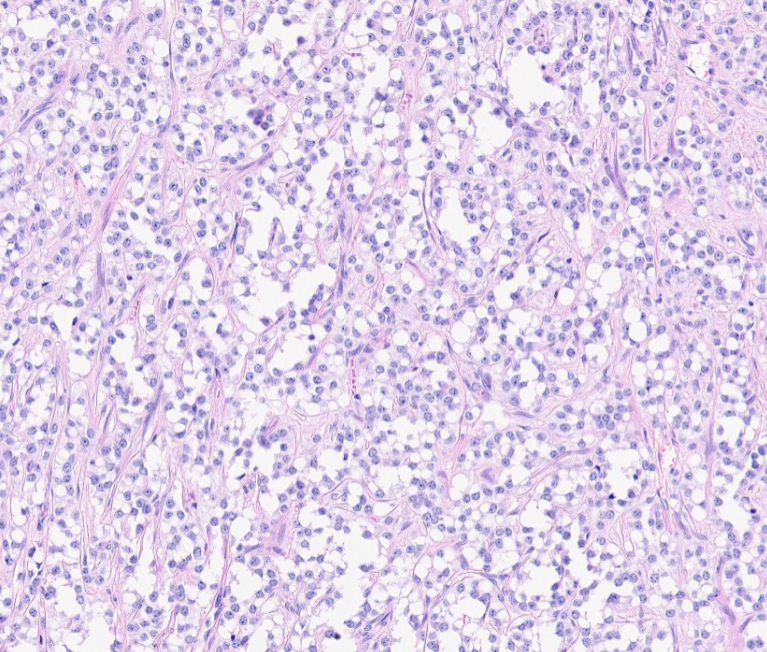
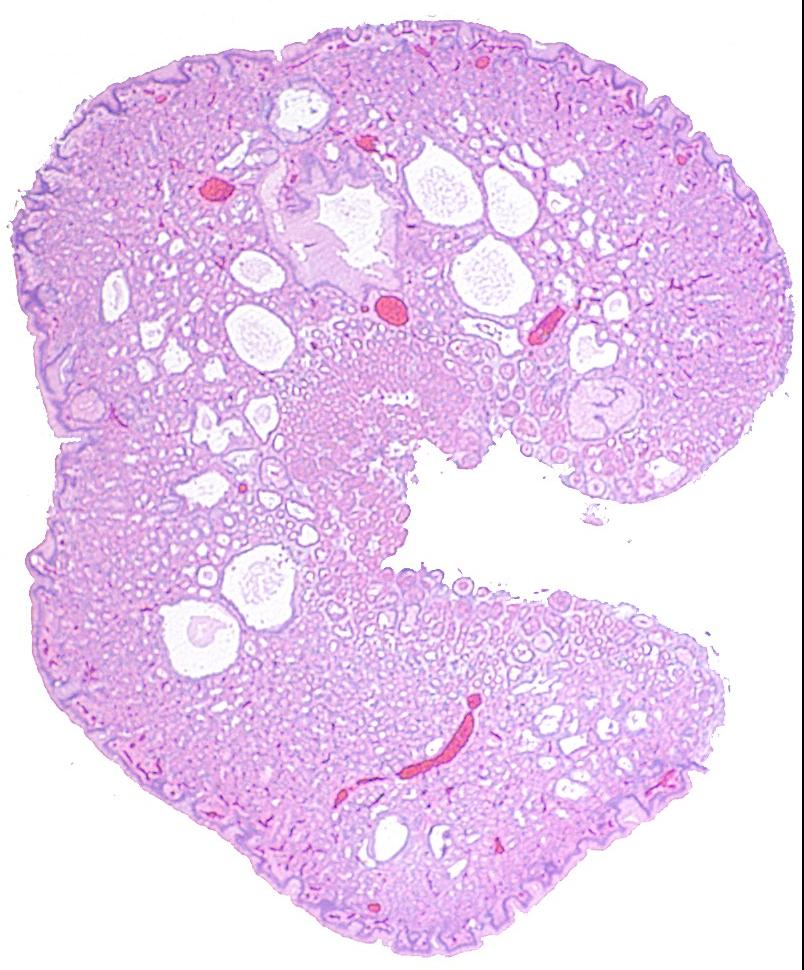
*Microcystic Stromal Tumor (MST) of the ovary*
Usually benign neoplasm with a classic triad: microcysts, solid cellular areas, and fibrous stroma.
IHC: Nuclear β-catenin, cyclin D1, WT1, and SF1 positivity
Key genetics: Mutually exclusive CTNNB1 or (less commonly) APC mutations
→ Rarely, MST is an extracolonic manifestation of familial adenomatous polyposis (FAP) and can serve as a sentinel event leading to the diagnosis of FAP
Dr. Parra Herran #USCAP2026#pathology#PathX#pathtwitter
Despite simplified diagnostic criteria, intraobserver and
interobserver variability remain in the interpretation of
colorectal serrated polyps
onlinelibrary.wiley.com/doi/10.1111/hi…#GIpath
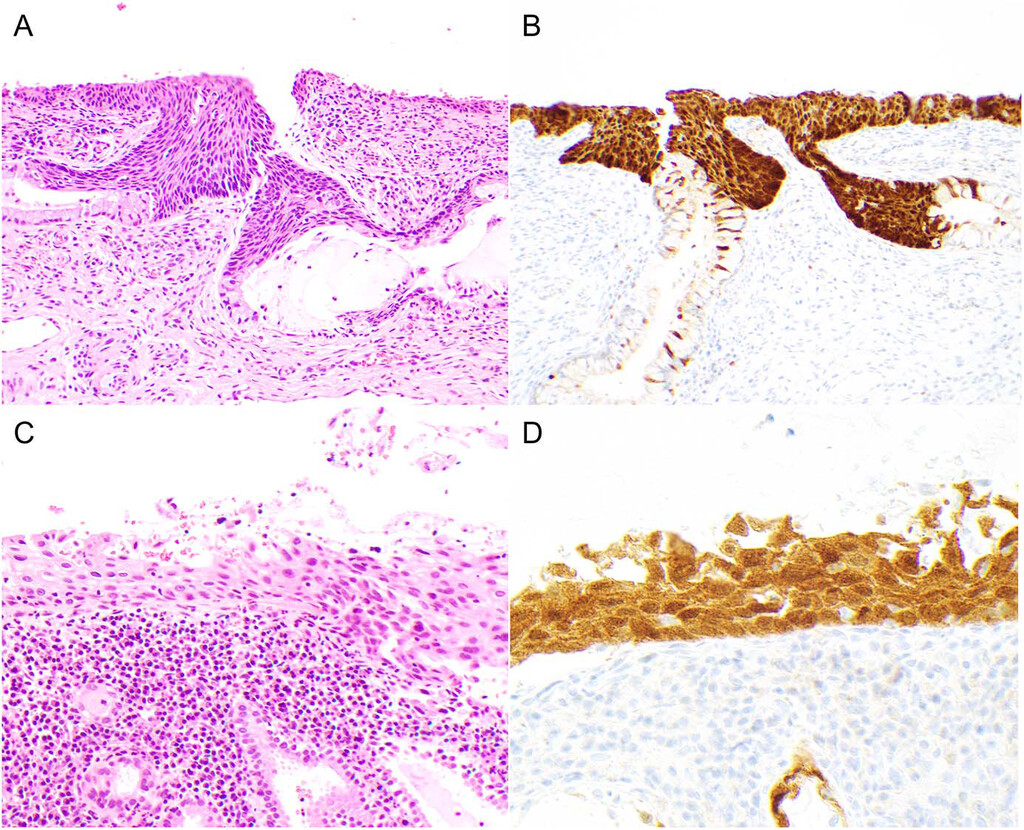
#PathQuiz 🔬
Clue in caption 🧐
A) Intraductal tubulopapillary neoplasm
B) Biliary intraepithelial neoplasia
C) Gallbladder carcinoma
D) Bile duct adenoma
#Pathology#GIPath@IARCWHO
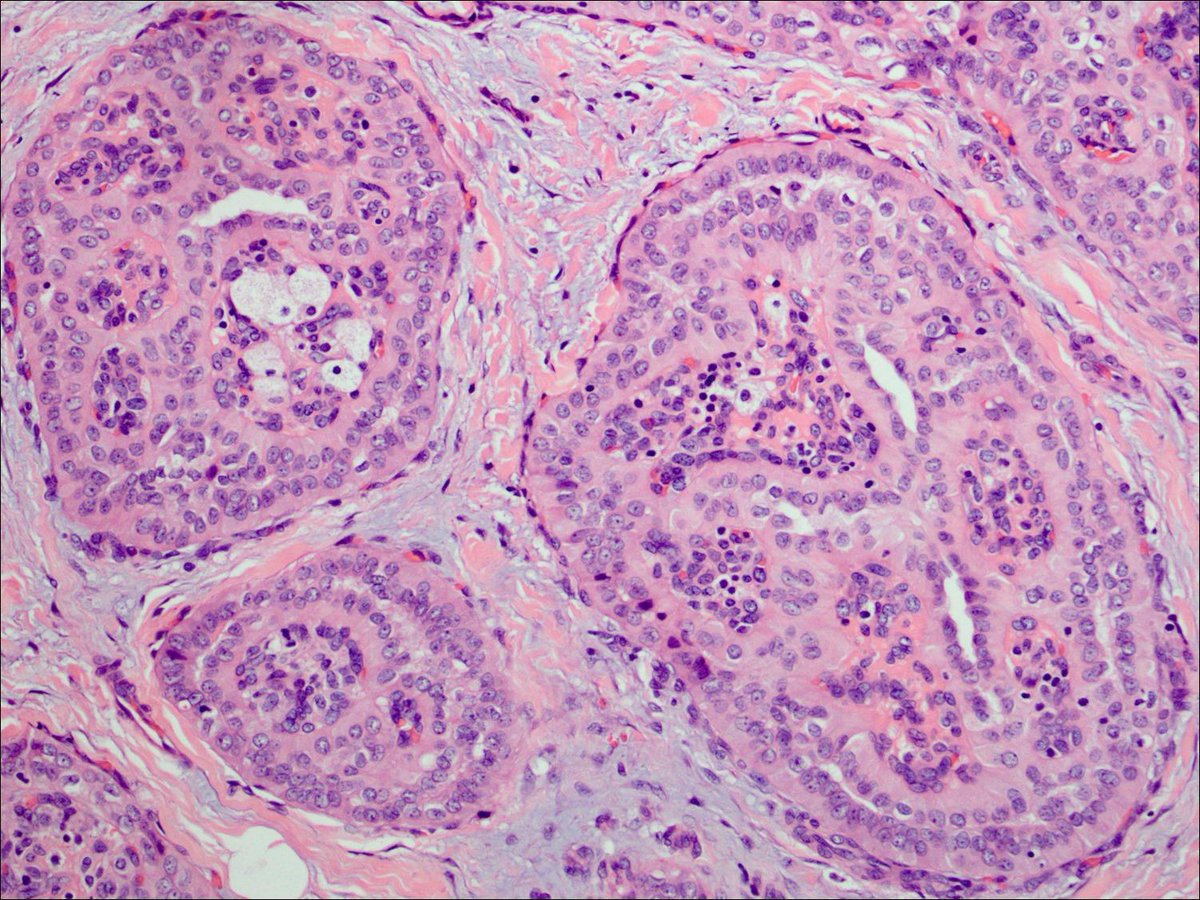
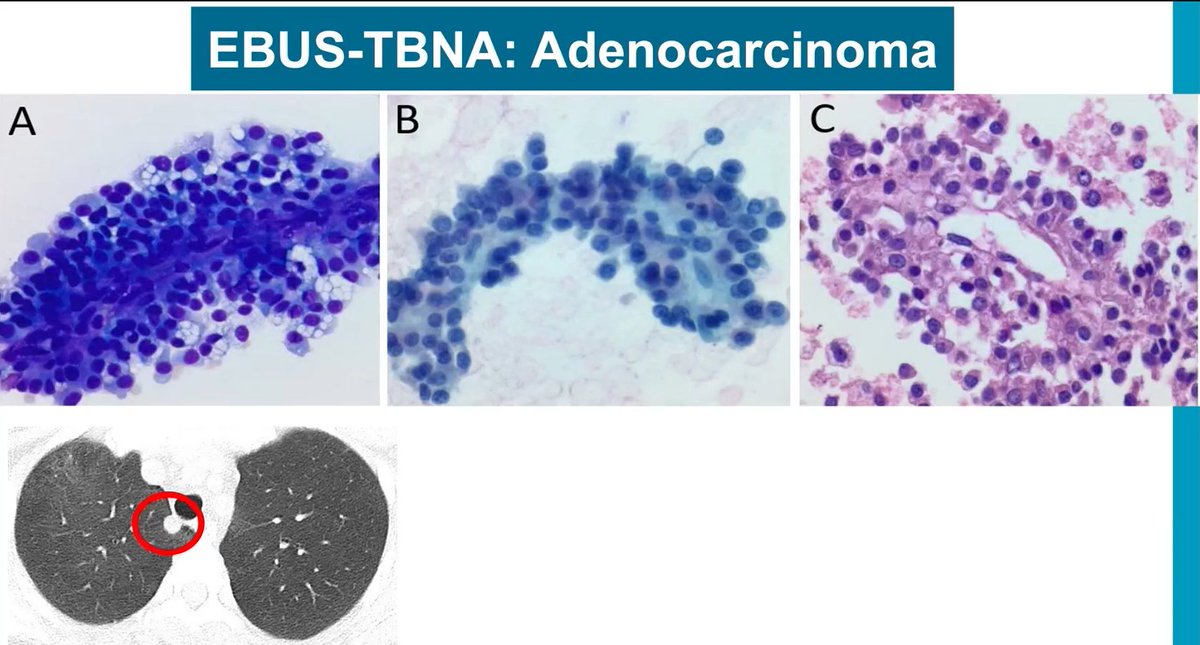
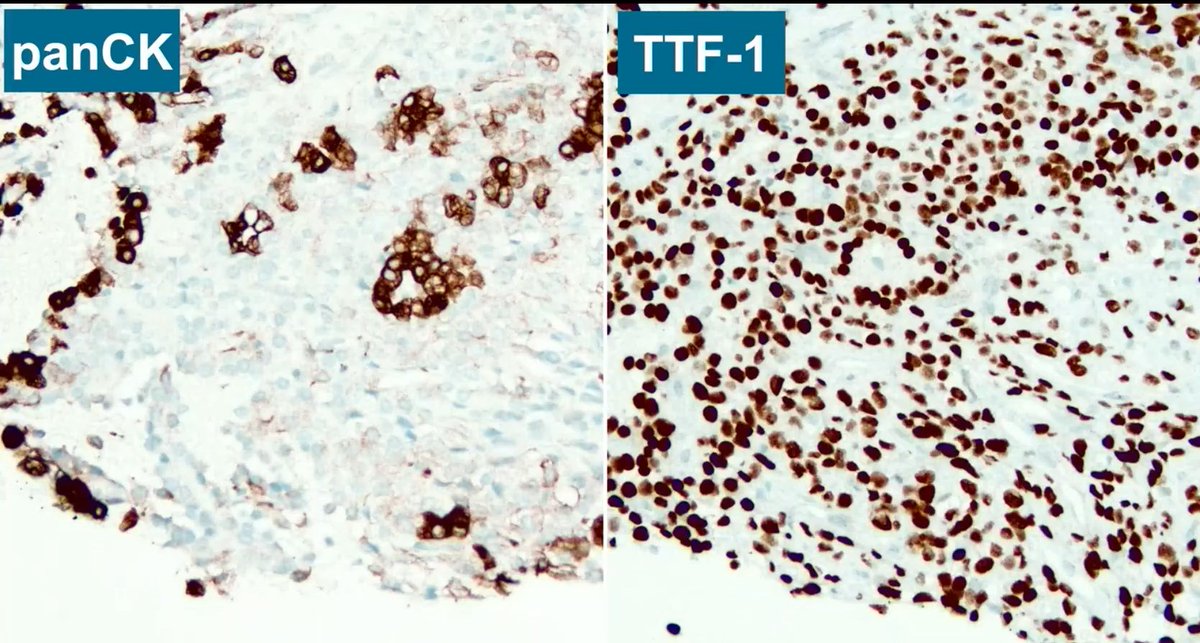
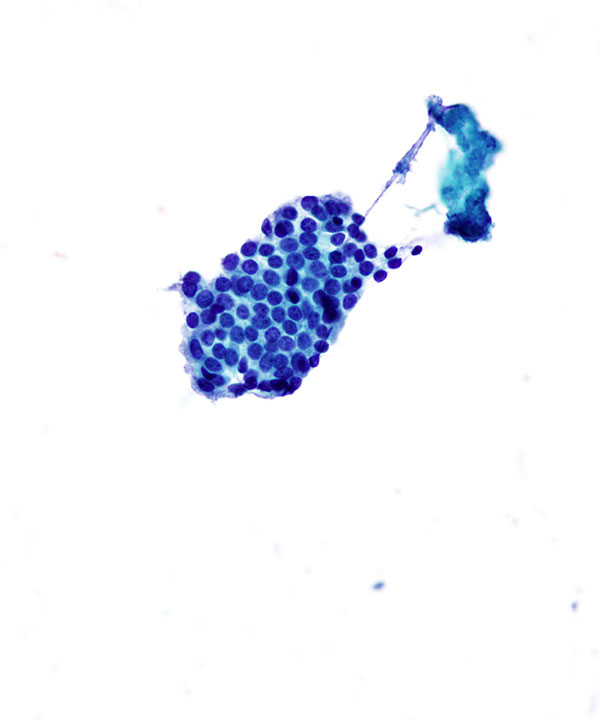
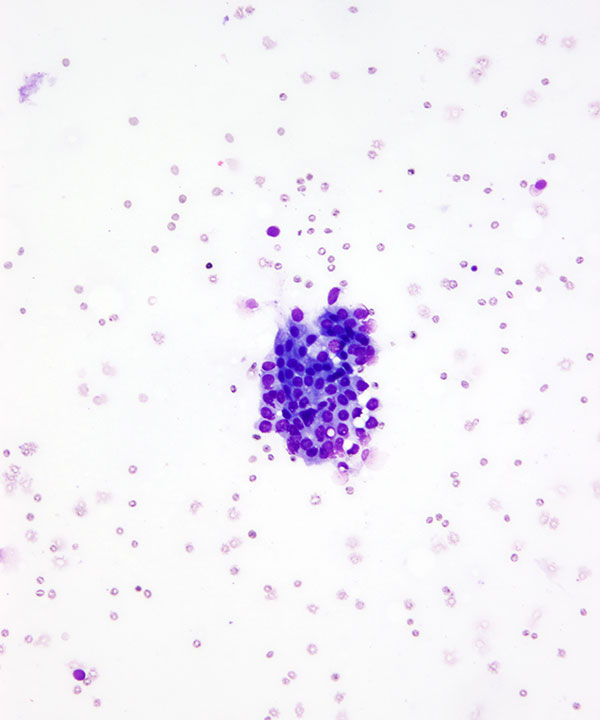
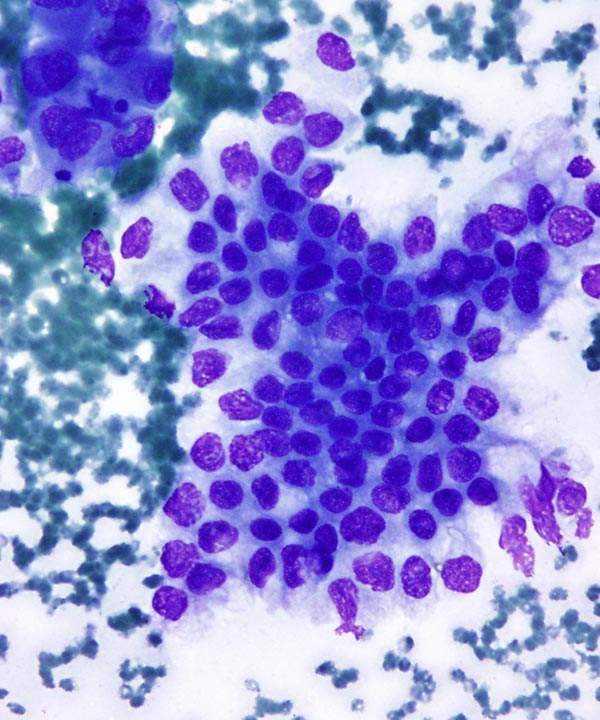
Common pitfall in lung cytopathology
Cytology mimicking adenocarcinoma (pic 1)
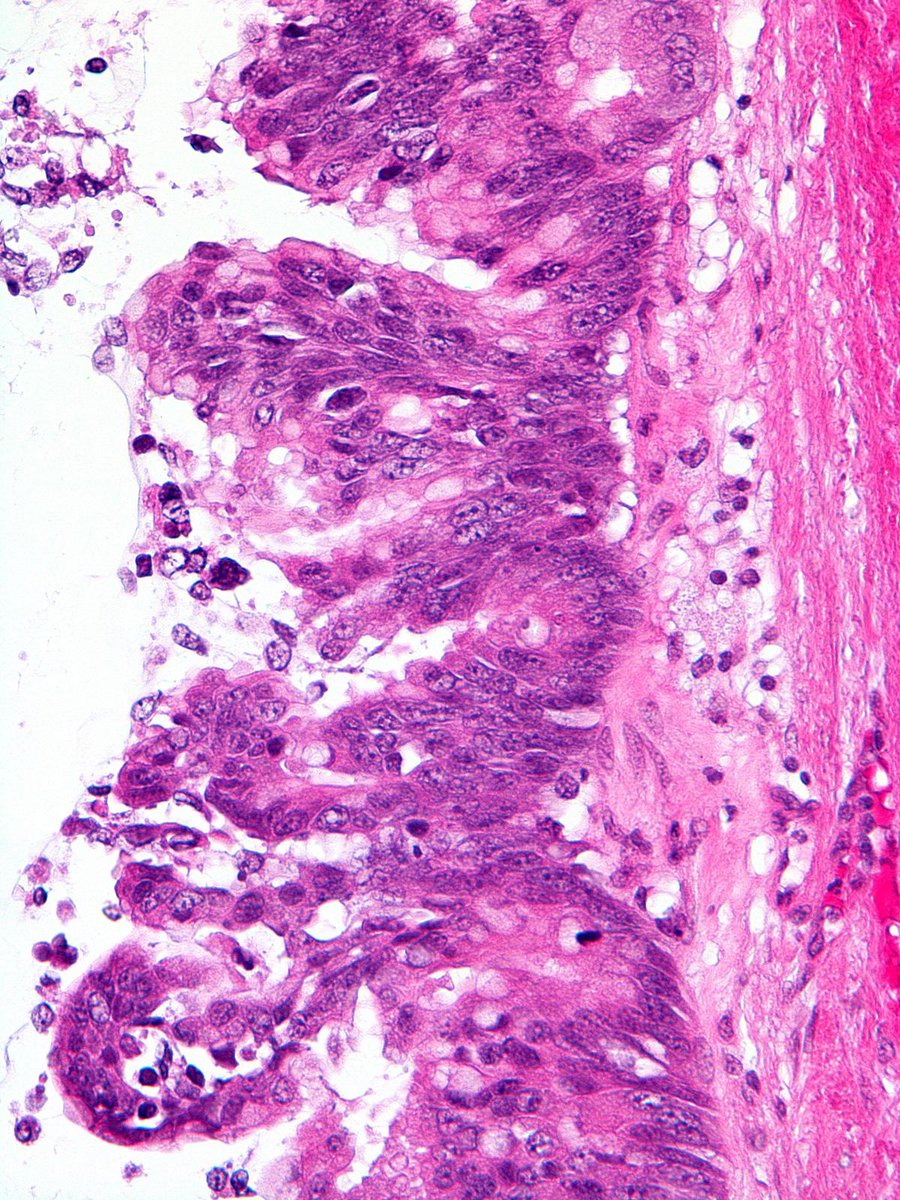
If you get a core biopsy and see a dissociation between CK AE1/AE3 and TTF-1 staining, stop!
Lung cells are not CK AE1/AE3 negative and TTF-1 positive; only stromal cells in sclerosing pneumocytoma are (pic 3).
Clues for sclerosing pneumocytoma in cytology (very hard diagnosis to make):
- Foamy macrophages, cuboidal cells, IHC (CK-, TTF-1+)
- Clinical clues: young to middle-aged women
Dr. Mukhopadhyay - Pathology on The Coast 2025, CAP On Demand #pathology#pathX#pathtwitter#CAP
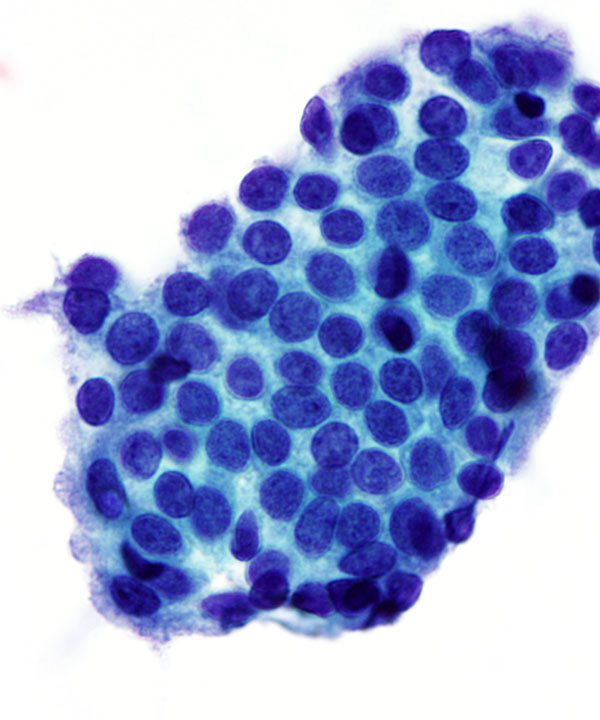
✅ Benign Ductal Cells 🎯
• Scant to moderate cellularity with cohesive two-dimensional flat sheets and honeycomb groups.
• Small uniform round to oval nuclei with smooth membranes and fine chromatin; nucleoli are inconspicuous.
• Myoepithelial or bipolar nuclei may be present and help support benignity; background is typically clean.
• Represents normal or reactive ductal epithelium; interpret atypia in clinical and radiologic context.
• 🐝 Honeycomb: Flat honeycomb sheet pattern of benign ductal cells.
Rare Presentations of Ovarian Tumors to Be Aware Of
High-grade anaplastic transformation of ovarian serous borderline tumor:
Most cases present as SBT with abrupt transition to a high-grade component, but one case presented as usual SBT with recurrence as high-grade component. Dismal prognosis.
Dr. Parra-Herran - Special Lecture: High-impact publications from the recent GYN path literature #isgyp#pathology#PathX
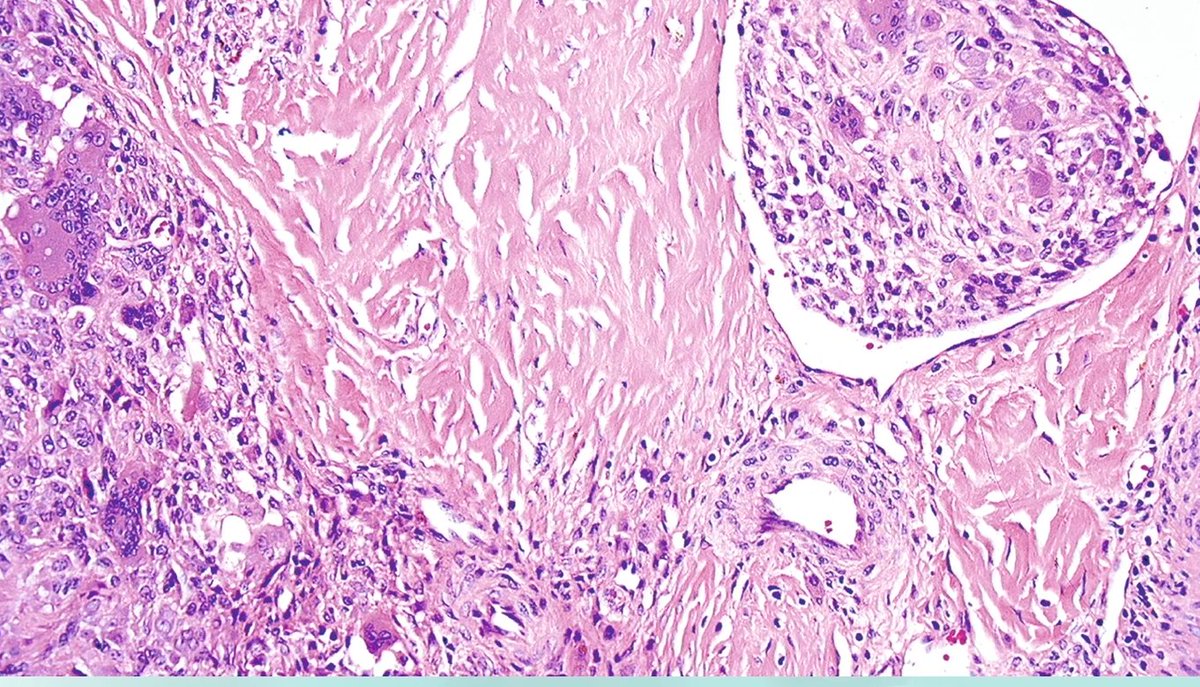
Tenosynovial giant cell tumor-"Atypical" features
The presence of these features (see list below) doesn't mean it is a malignant tumor -pitfall 🛑
-Vascular invasion (pic 2)
-Bone involvement (pic 3) but no histologic features of malignancy
-Extraarticular location (pic 4)
Dr. Nielsen-Neoplastic and Non-Neoplastic Lesions of the Synovium #USCAP25#PathX#BSTpath