Sabitlenmiş Tweet

Thanks for the votes
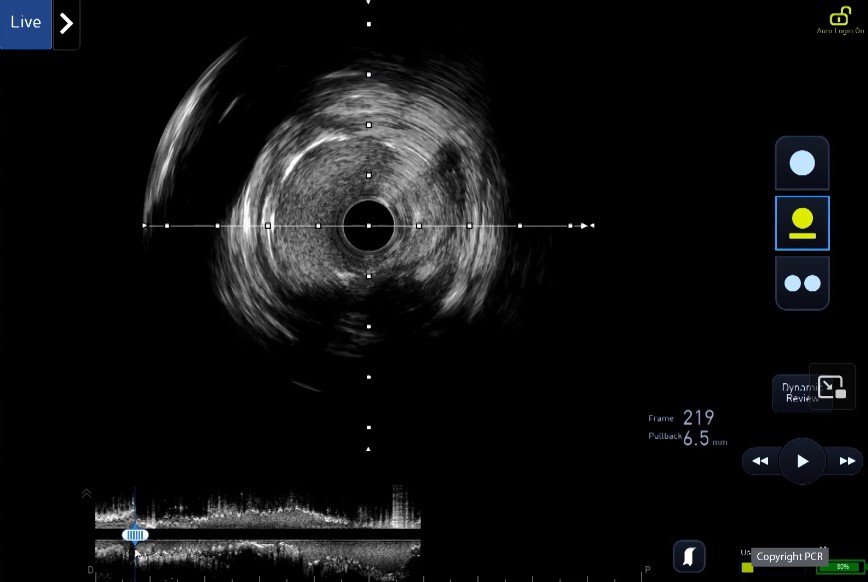
🎯 We need to clarify if Os LAD/LM are involved or not (most of the time yes)
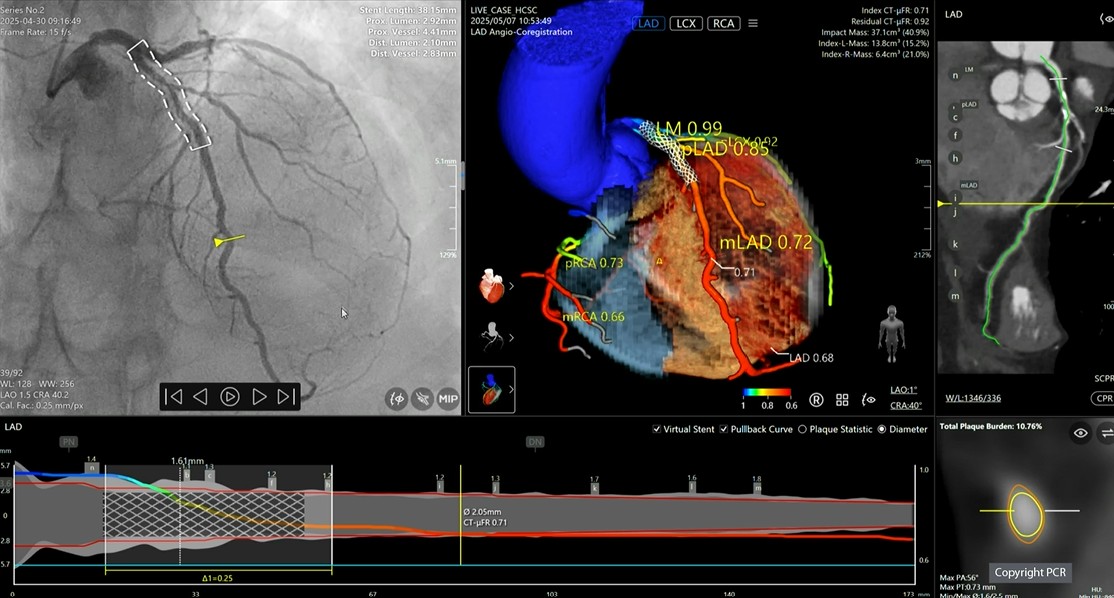
🎯 Having multi modality imaging including CTCA and OCT helps.
🎯 Decided to nail Os but with AI using the co-registration feature



English