Severe TR with IVC/HV systolic flow reversal
English
Carlos El-Tallawi, MD, FACC, FASE
1.5K posts

@HeartToProve
Conscious lump of atoms posting edutaining tweets | AUBMC cardiology | Houston Methodist Multimodality CV Imaging | Echo + CMR | Valvular heart disease — MVP



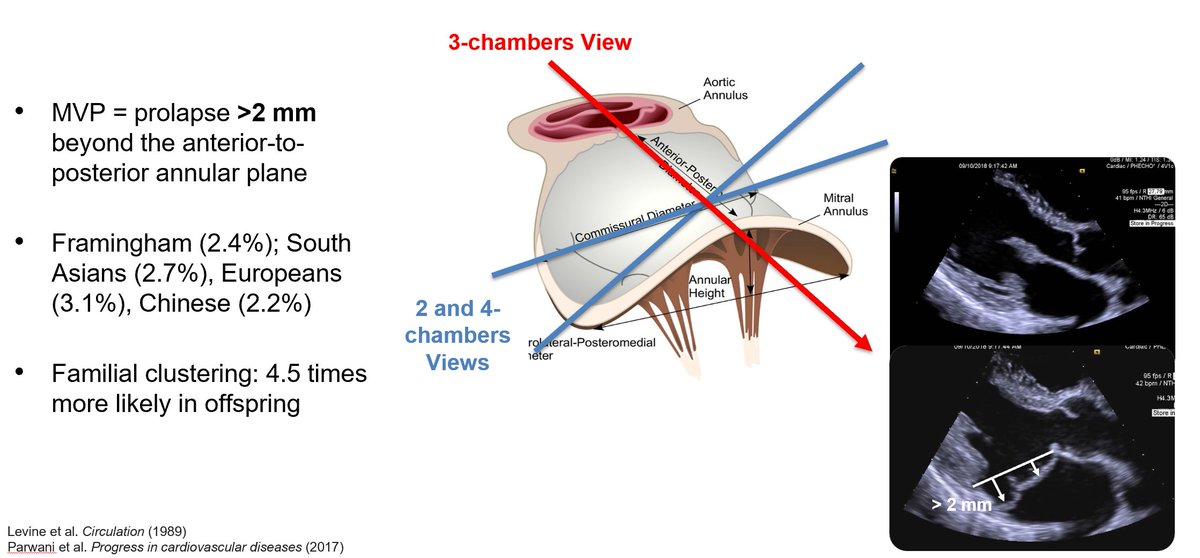
@PWesslyMD @LucySafi @PriyaPanday27 @NadeenFaza @ASE360 @JournalASEcho Our group also identified a novel Doppler sign —Bifid-E wave— that could represent an additional echocardiographic marker of advanced MVP and myocardial fibrosis. Keep an eye out for this next time you're reading a Barlow Echo. #ASEchoJC

@PWesslyMD @ASE360 @JournalASEcho Very important -- flail =/= severe MR! In our data a flail leaflet had 81% specificity for severe MR as defined on CMR >60 mL/50% #ASEchoJC