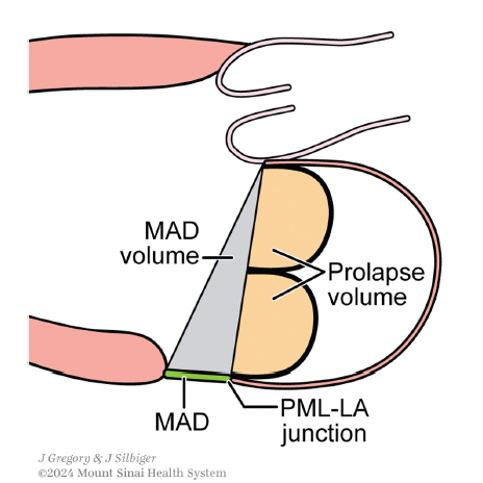
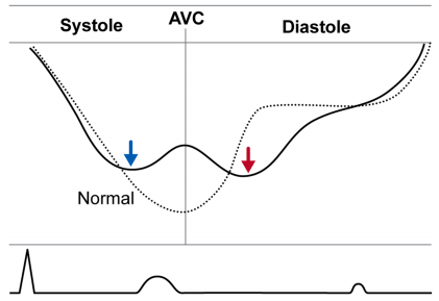
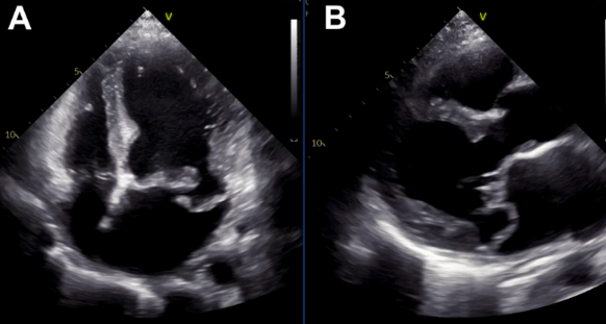
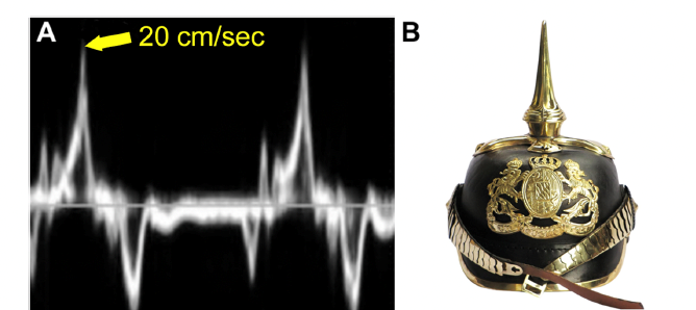
Superior displacement of the mitral valve into the LA increases traction exerted on the papillary muscles. As a result, the myocardium beneath the papillary muscles is pulled into the LV cavity. This causes the LV crest as well as the posterior annuus and the attached posterior leaflet to rotate (as a unit) in the counterclockwise direction. This motion is called curling. Papillary muscle traction also pulls the basal posterior wall in the apical direction. This brisk motion causes a prominent s’ wave on tissue Doppler imaging. An s’ > 16 cm/s is called the Picklehaube sign. #ASEchoJC
English