BREAKING: Camp Mystic, an all-girls summer camp on the Guadalupe River, has confirmed that all 27 campers and counselors lost their lives in the devastating Texas floods.
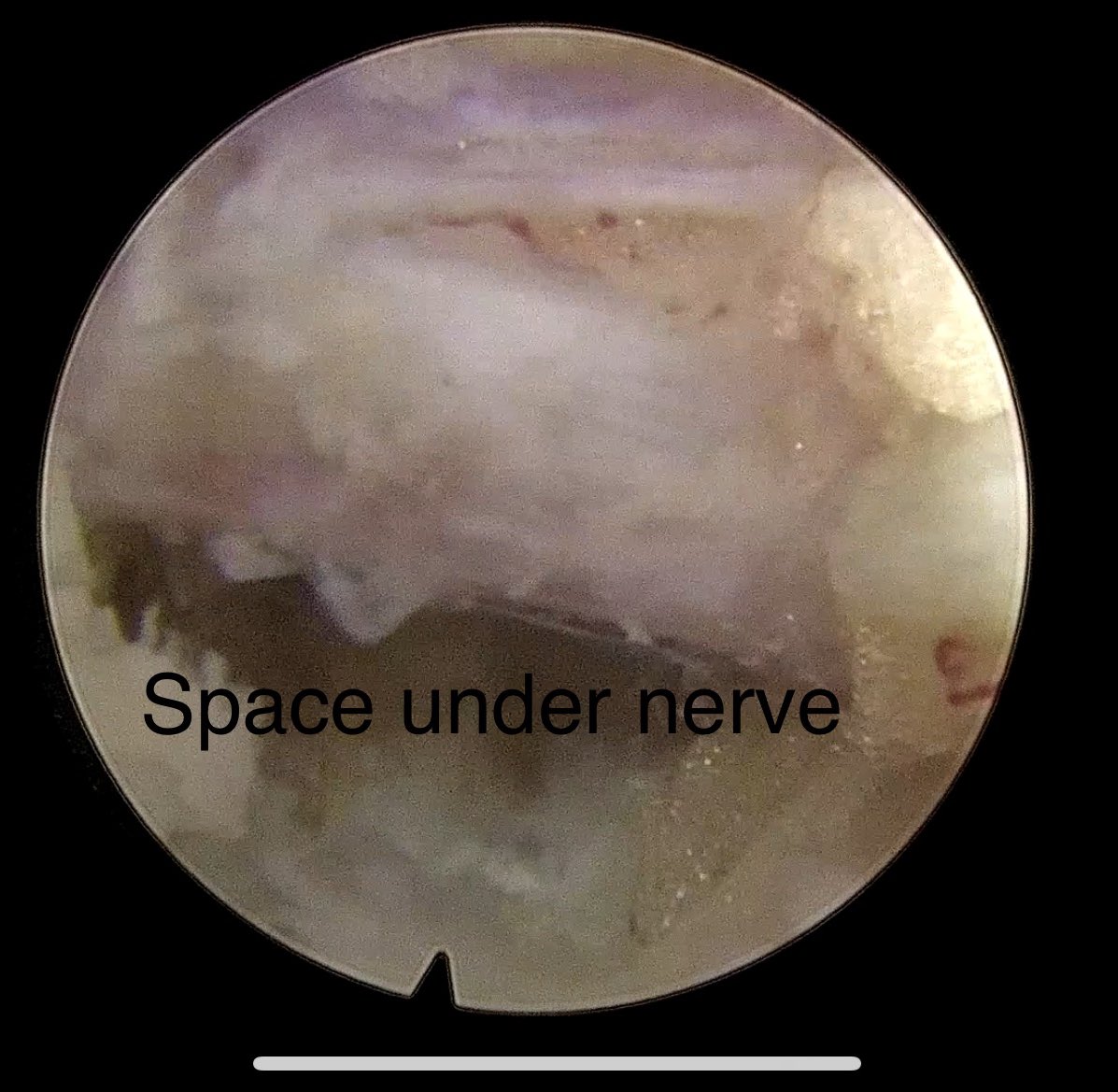
Images and video from recent endoscopic spine case. Amazing that this can be done thru 1cm incision and no bone removal. An amazing option for patients. I'm happy to offer this option!
9F with enlarging cerebellar mass radiographically consistent with LGG. Underwent stereotactic biopsy followed by single catheter LITT @PhxChildrens@barrowpch. Home POD1.
2nd Tumor Symposium (first in 2023) and the 1st meeting of our new Society! We've got a fantastic group of speakers and topics with attendees coming from all over the world! Only a few spots left. If interested, please contact me: pklimo@semmes-murphey.com.
@HarshDeora You absolutely do not want to skeletonized the MCA from the bifurcation because of the lenticulostriate perforator. You want to skeletonize only within lateral aspect of the sylvian fissure where the vessel lies on top of the insula
@HarshDeora These are one of the more challenging tumors to remove. I believe the only way to get a complete resection is with intraop MRI, but that's not available in most places. You can see you left tumor in the temporal stem and there is a perforator infarct of the head of caudate.
@MarkD_Jr@KyleWuMD@guilherme_fngr@JoshVignolles@NeurosurgeryOSU Your conclusions make perfect sense and what one would expect. However, your use of the term "Case Control" is incorrect. This is not a case control study. It's a retrospective cohort. "Case Control" is often used incorrectly within neurosurgical literature.
We are often faced with the question of how best to manage residual tumor after a bx or subtotal resection of a GBM deemed inoperable. Past studies have shown completion resection of these lesions is safe, but does it provide oncologic benefit?
journals.lww.com/neurosurgery/f…
One of the hardest tumors I’ve tackled in a long time. 2 year-old male presents with vision loss and sleepiness. Biopsy shows adamantinomatous craniopharyngioma. Subfrontal approach. Encasing every major neurovascular structure of the skull base. Was able to take it back to the hypothalamus, the chiasm, and dissect off the nerves and vessels. Likely stage 2 transcallosal from the top needed. Thinking about toci/avastin. Thoughts? @PhxChildrens@BarrowNeuro
2/2 Nothing comes close to the impact of having 1 or more postop event (POE) - an increased odds of almost 30 fold!! While you can't predict everything that happens after surgery, there are definitely some that you can anticipate and prepare for! pubmed.ncbi.nlm.nih.gov/39612129/
1/2 When I started @LeBonheurChild & @StJude almost 15 yrs ago (😳), one of the first things I did was set up a number of prospective databases. In what will hopefully be a trilogy of papers, we first looked at predictors of extended LOS (>7days) after elective craniotomy.
Excited to announce the 2nd Tumor Symposium and the 1st meeting of the new Society for Pediatric Neurosurgical Oncology @ St Jude campus! Please reach out if interested in attending. A day and a half of fantastic speakers, a variety of topics and controversies to get into.
Shunt checklists are commonplace in pediatric neurosurgery. One key component is limiting OR traffic. Does it make a difference? While we couldn't answer that question, we did look at who came in and out of the OR in 50 cases with surprising results.pubmed.ncbi.nlm.nih.gov/39576978/
Will start posting our projects as they get published, more to give recognition to all those that contributed to the process. I welcome any and all comments and criticisms. Let me know what you liked and disliked about our work. @MemphisNSGY
Around the time COVID hit, I pulled back a bit on research and writing for a number of reasons. I had lost some of the excitement and passion. I feel the energy and desire returning...
Had a great time at #cns2024 directing the epilepsy surgery symposium with Kurtis Auguste MD and @RolstonJohn! We had a fantastic lineup of speakers covering all aspects of epilepsy surgery from pediatrics to adulthood! Got to see great friends @TaylorAbelMD and others!
What an incredible honor it was to host Dr. Jeff Blount as our 2024 Talley Family visiting professor. A giant in our field whose impact will be felt for many years. A kinder and more humble soul you will not find. On behalf of @MemphisNSGY, a heartfelt thank you, Jeff.
@aviagajjar@NeurosurgeryCNS So if you knew you or a loved one were gonna have a TBI, and you were given a choice when, would you choose the end of June or beginning of July? I know my answer...
Our analysis of 3.2M TBI patients in @NeurosurgeryCNS shows no “July Effect” 🚨🏥🧠. Admissions in July have lower mortality and complication rates, showing that teaching hospitals maintain excellent levels of care year round. #Neurosurgery#TBI#JulyEffect
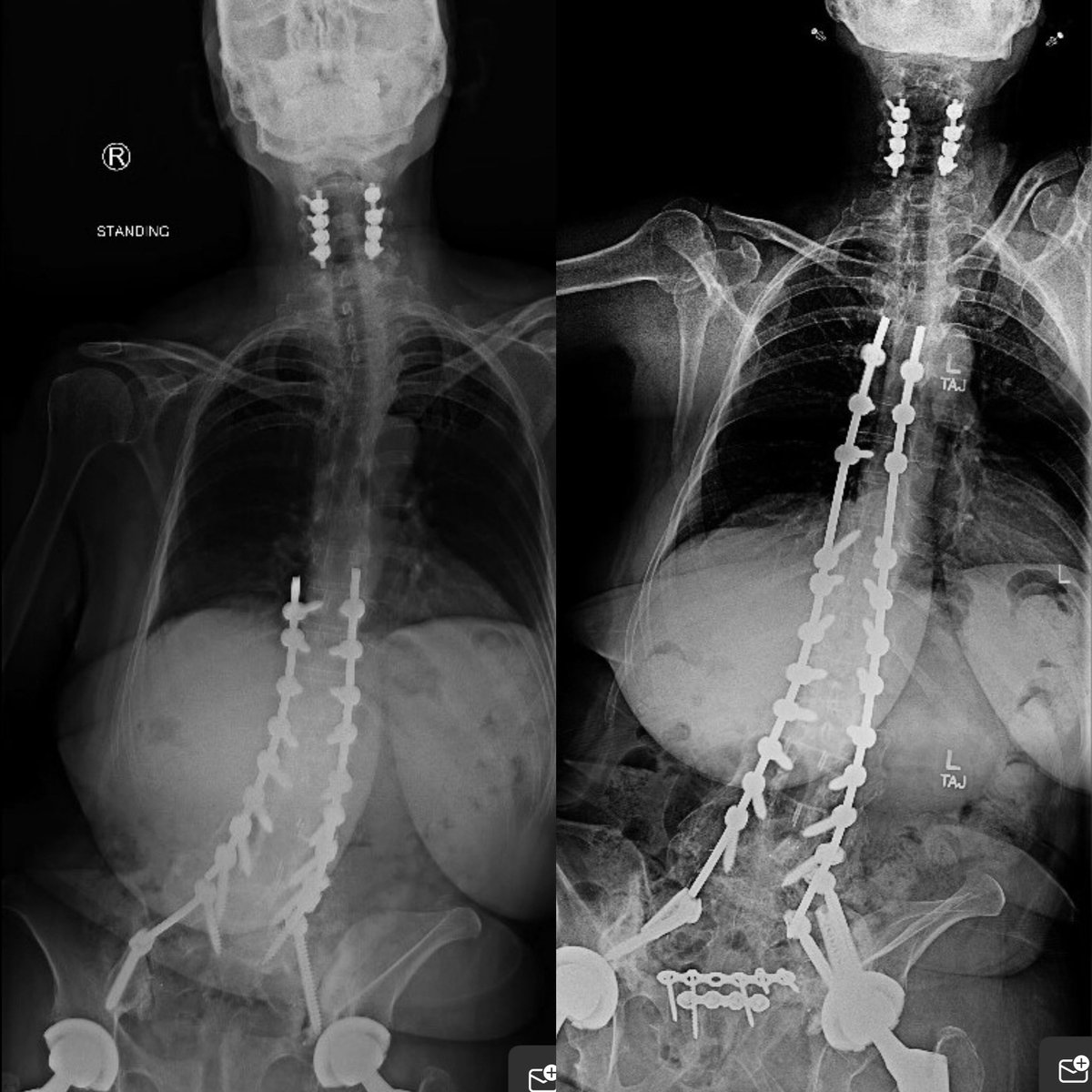
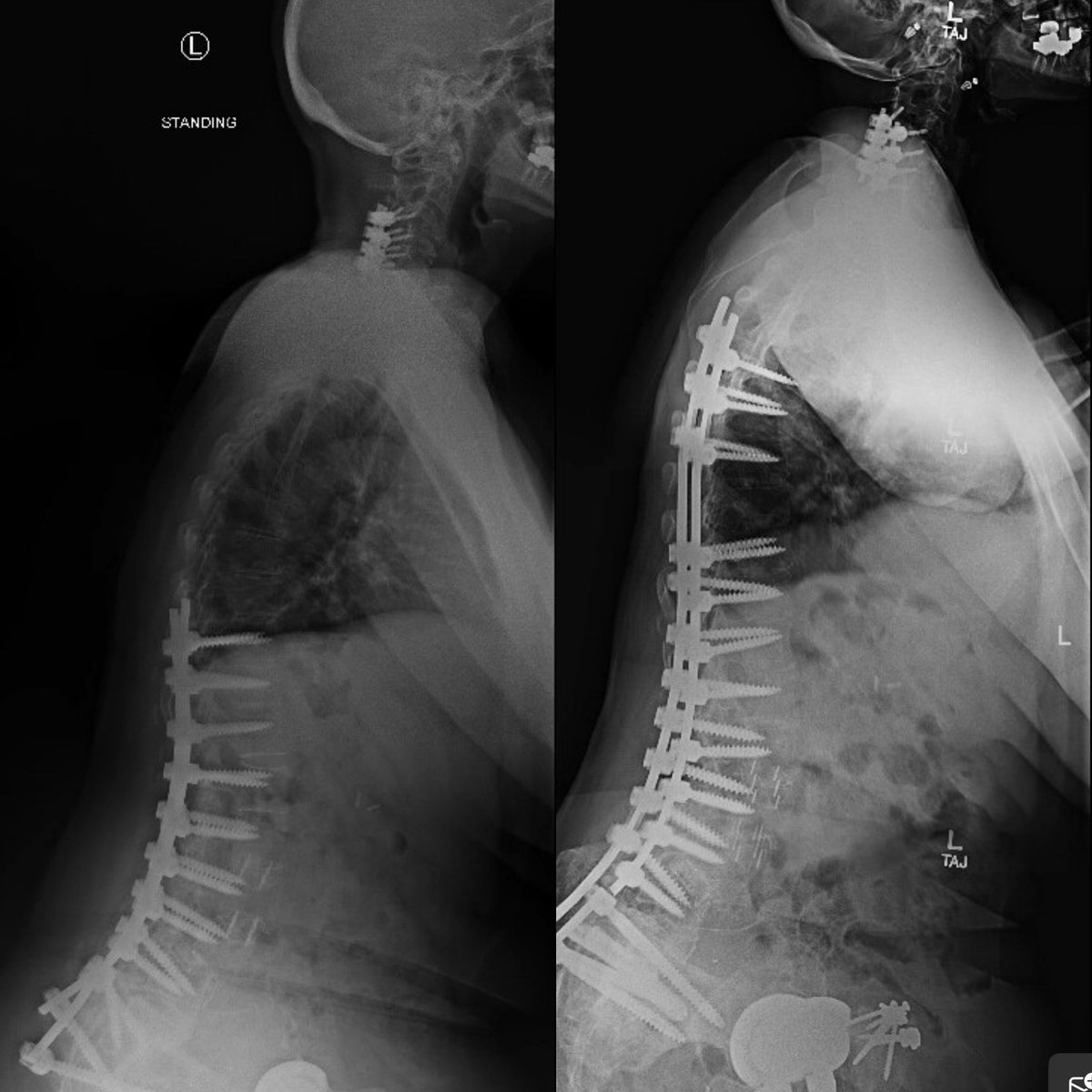
67 yo F with a T10-pelvis fusion who underwent an attempted revision surgery at outside facility. Has ongoing coronal imbalance, a backed out cage at L4/5, PJK with lucency at T6, and pelvic instrumentation failure. Back pain and radiating L leg pain. What’s your approach here?