Thanks @ARRS_Radiology#ARRS26 for this ‘Gold medal award’. Truly motivating for me as well as inspiring for other radiologists. Really appreciate the honor.
1/
🧬 CTLA-4: The Checkpoint That No One Believed In
In the early 1990s, James P. Allison, an immunologist at UC Berkeley, was studying T cells when he stumbled upon CTLA-4 — a molecule thought to activate T cells, just like its cousin CD28. Most scientists believed it was just another co-stimulatory signal.
But Allison suspected otherwise.
“It was like everyone saw a brake and called it a gas pedal.” – James Allison
He did something few others had tried: he blocked CTLA-4 in mice with tumors and saw an explosive immune response — the tumors melted away. Proving that - rather than stimulating immunity, CTLA-4 was a brake on T cells.
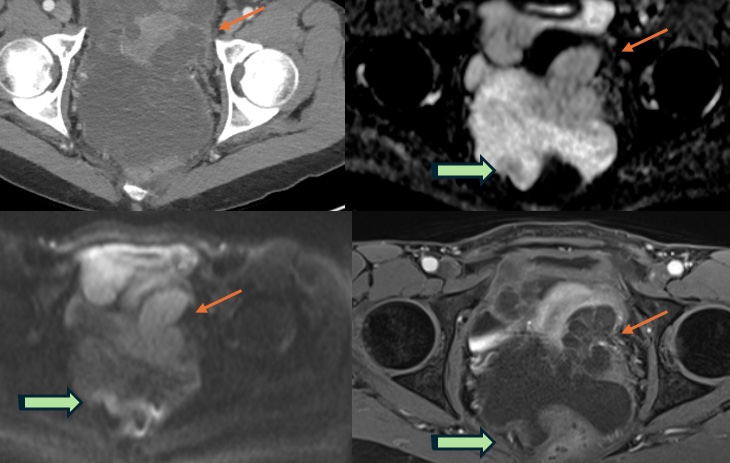
Bladder cancer – key risk factors & behavior:
• Smoking is the most important risk factor 🚬
• Exposure to aniline dyes, as they are metabolized in the liver but excreted in urine
• Among subtypes, papillary urothelial carcinoma is more common and generally less aggressive than non-papillary subtypes
Bladder diverticula carry a risk of malignancy due to urinary stasis.
Teaching pearl: diverticulum
Bladder diverticula lack muscularis propria
→ earlier extravesical spread
→ staging pitfalls & worse behavior
Does this diverticulum look sinister?
#Radiology#BladderCancer#UrothelialCarcinoma
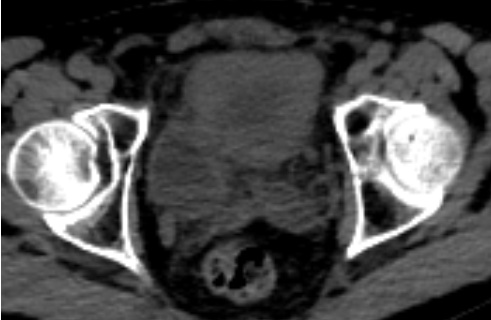
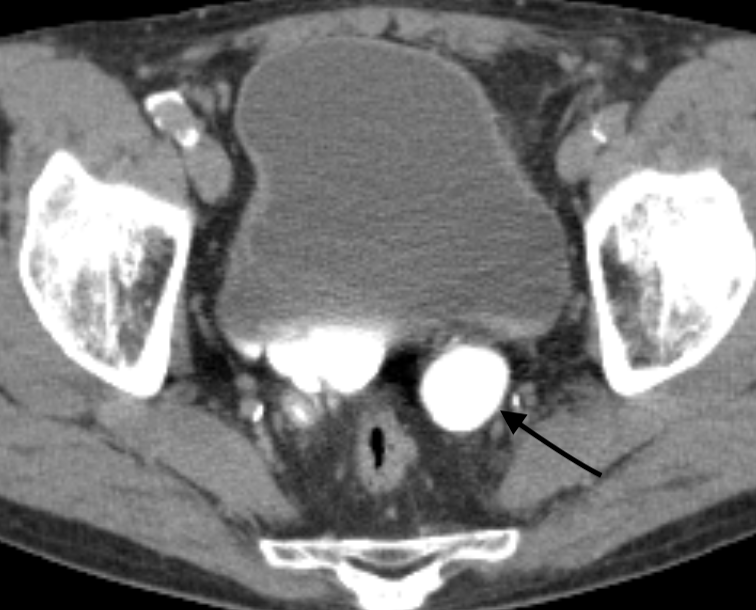
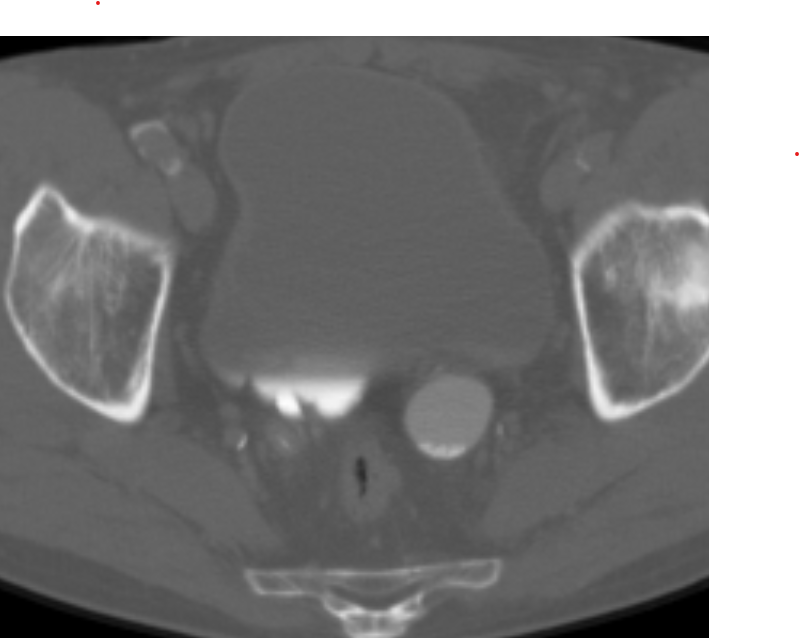
Can you spot what lies within the dilated left ureter (black arrow)?
In the absence of a non-contrast phase (as in many trauma studies), switching to the bone window can be helpful -- like in this case, it clearly reveals multiple ureteric calculi that were otherwise inconspicuous.
A small window change—big diagnostic payoff 🦴✨
#Radiology#CTtips
My article "Should I have become a radiologist? The hype versus reality of radiology AI, AI in general and the road ahead" .
It is based on my recent talk for @REF_INDIA with a few additions.
It is intended for medical students considering a career in radiology but facing a barrage of “AI will replace radiologists” fear mongering and for radiologists and radiology trainees seeking a distilled overview of the state of radiology AI today and what to expect going forward.
Link in 🧵
This might be the most disturbing AI paper of 2025 ☠️
Scientists just proved that large language models can literally rot their own brains the same way humans get brain rot from scrolling junk content online.
They fed models months of viral Twitter data short, high-engagement posts and watched their cognition collapse:
- Reasoning fell by 23%
- Long-context memory dropped 30%
- Personality tests showed spikes in narcissism & psychopathy
And get this even after retraining on clean, high-quality data, the damage didn’t fully heal.
The representational “rot” persisted.
It’s not just bad data → bad output.
It’s bad data → permanent cognitive drift.
The AI equivalent of doomscrolling is real. And it’s already happening.
Full study: llm-brain-rot. github. io
Beautiful example of fat containing inguinal hernia and Inguinal canal lipoma co existing. Remember ICL connects to extraperitoneal fat.
#FOAMrad#abdrad#radiology#radres
Great group! Casual social last evening to welcome our growing cohort of @ABR_Radiology#AlternatePathway fellows here @CURadiology. Thanks to our terrific program coordinators & PDs who support them in their unique journeys in #RadEd!
#RadCommunity
11/
📷 Why Imaging Follow-up Matters
Unlike older criteria, new or enlarging lesions post-immunotherapy do not automatically mean progression.
✅ Follow-up imaging is crucial
⏳ It confirms whether it’s pseudoprogression or true progression
🗓️ Always re-image after 4+ weeks before changing treatment plans.
10/
🕒 Immunotherapy Response ≠ Immediate Shrinkage
Clinical responses to immunotherapy can be delayed — what appears as tumor growth might not be true progression.
📌 Key Point:
Wait for two follow-up scans, at least 4 weeks apart, before concluding progression or failure of therapy.