KYULE retweetledi

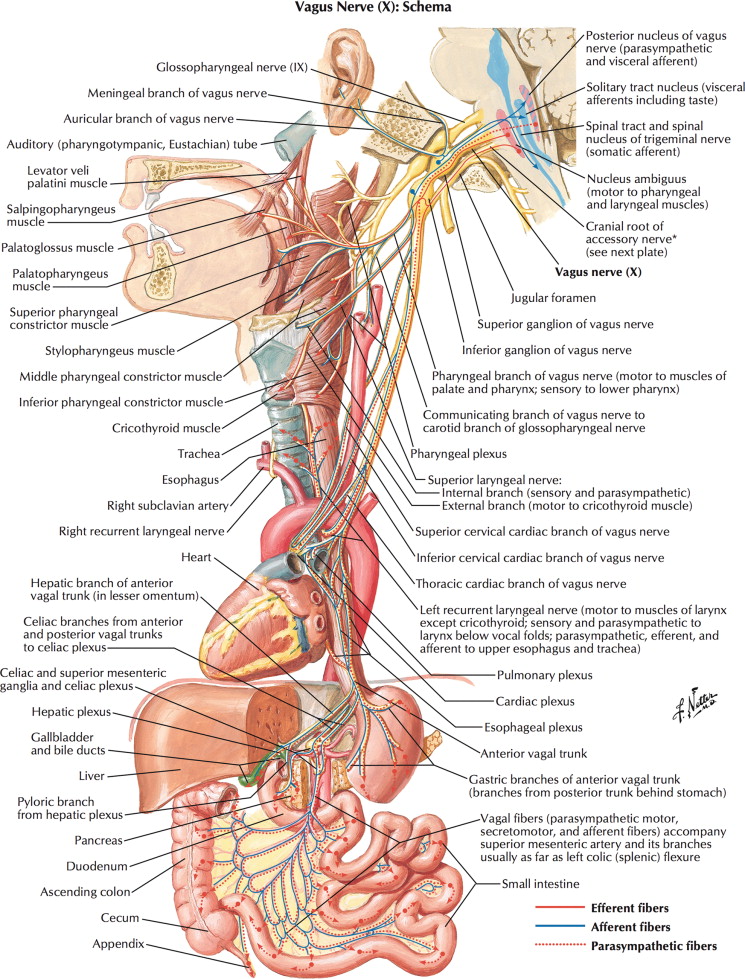
What is the description or diagnosis or Differential?

English
KYULE
18.3K posts





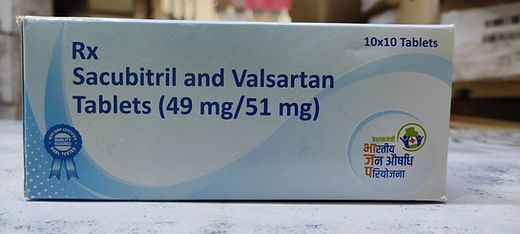






Which organ damage causes this?



Very sad situation here🥲 It is 1 PM It's now 4 hours. Terrible 💔



What informs your allocation or it's just coz you "feel" 🤣