Mohamad Bakhaidar retweetledi

الوافد مكسب قصير المدى لسوق العمل ، لكنه لا يصنع اقتصادًا مستدامًا وحده. التوازن الصحيح يكون بربط استقدامه بنقل معرفة حقيقي، وتكلفة عادلة، ومسار واضح لإحلال الكفاءة الوطنية دون تعطيل لسوق العمل .

العربية
Mohamad Bakhaidar
5.5K posts


@MBakhaidar
Neurosurgeon | Spine Surgeon Spine Surgery Fellowship @MCWNeurosurgery - Neurosurgery Residency @McGillNeurosurg - Future Neurosurgery Faculty @KAUHospital


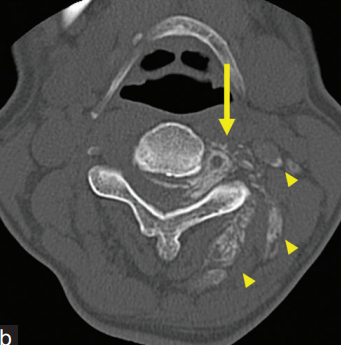
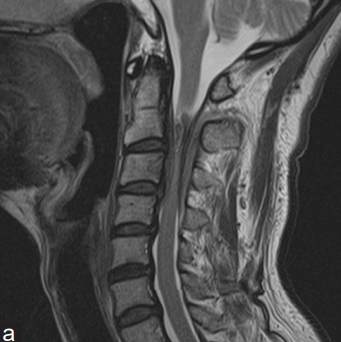
#إنجاز_طبي فريق طبي في #مدينة_الملك_فهد_الطبية يعالج حالة نادرة لطفل يعاني من تشوه وريد دماغي، حيث أُجريت له قسطرة دماغية دقيقة وزُرعت دعامة وريدية، في إنجاز يُعد نادرًا على مستوى الشرق الأوسط. #تجمع_الرياض_الصحي_الثاني
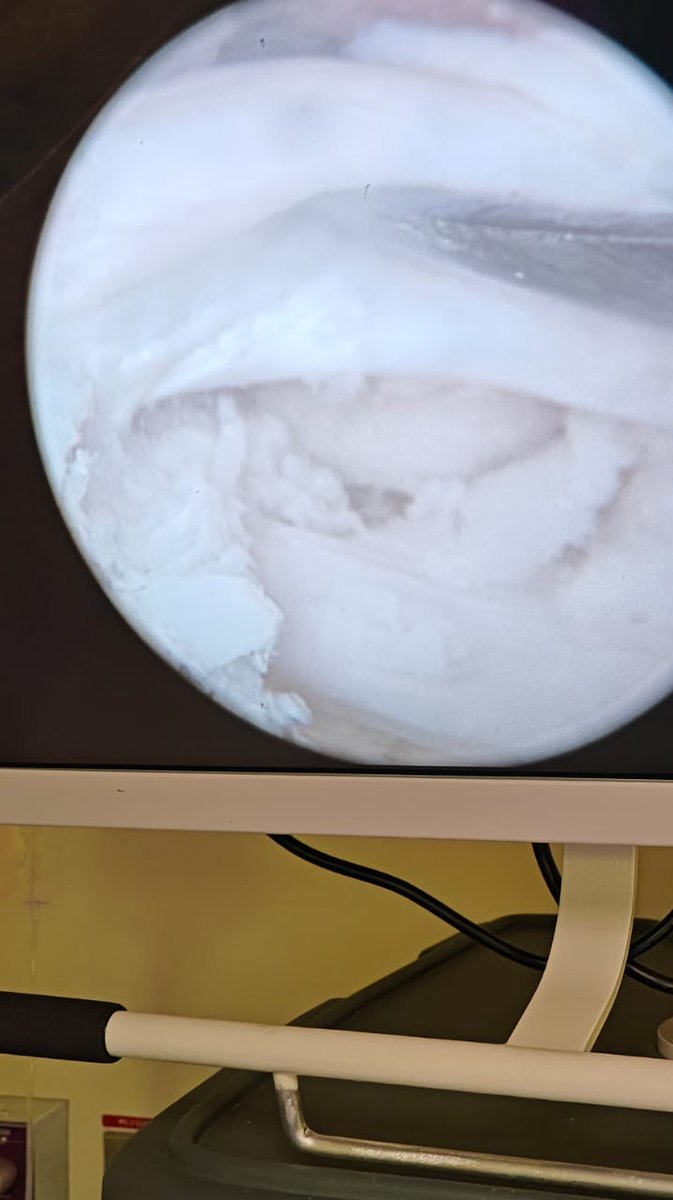
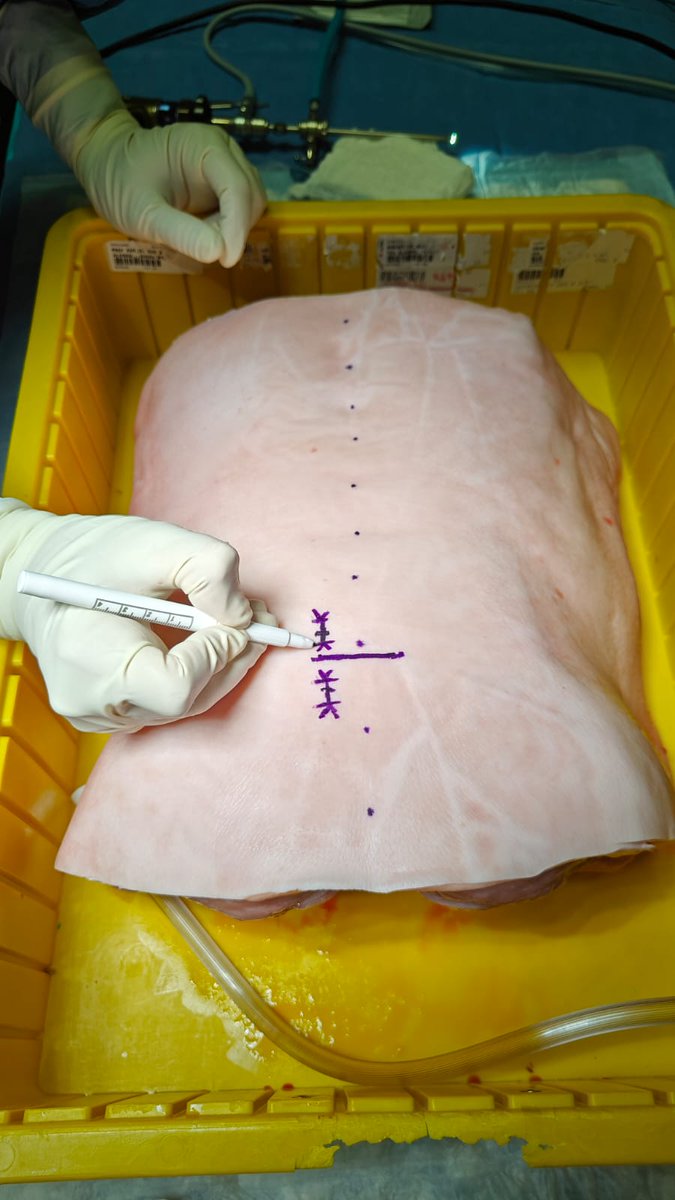
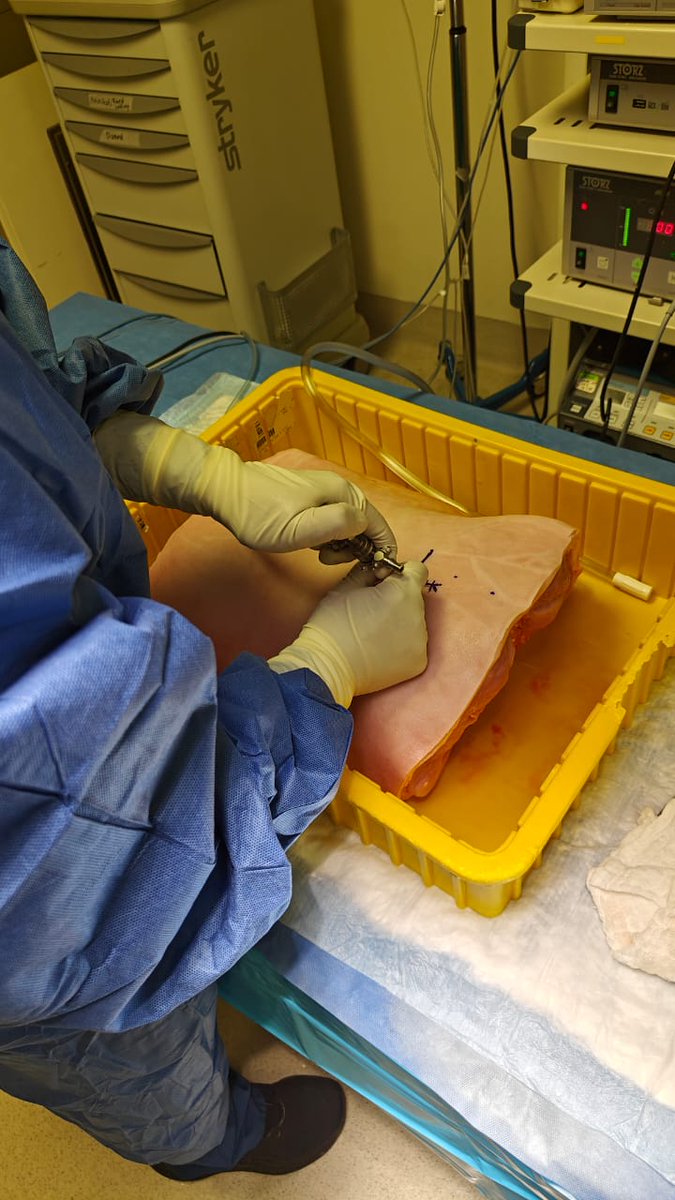
New pub: rdcu.be/emUKX Minimally invasive laparoscopic and robotic anterior lumbar interbody fusion. In quest to minimize the ‘surgical footprint’, these techniques may help. @DukeMedSchool Isa Decker @MBakhaidar , Summer Shabana, Meriem Boukhiam, Sabino Zani