💧 DKA resuscitation: Normal Saline vs Ringer’s Lactate, does it really matter?
For decades, 0.9% NaCl has been the default fluid in diabetic ketoacidosis.
But… is it still the best choice?
🧪 New randomized ICU data (2025-2026)
👉 88 patients with severe DKA
👉 Ringer’s Lactate (RL) vs Normal Saline (NS)
👉 Same insulin protocol
📊 Primary outcome: DKA resolution at 48h
➡️ No difference
• RL: 56.5%
• NS: 50%
(p = 0.66)
⚖️ So… clinically equivalent? Not exactly.
The physiology tells a different story 👇
🧠 What RL does better
Compared to NS:
✔️ Higher bicarbonate early
✔️ Better potassium levels
✔️ Lower chloride at 48h
➡️ Translation:
• Less hyperchloremic metabolic acidosis
• Lower risk of hypokalemia
• More physiologic acid-base recovery
⚠️ What NS still does
❗ Same DKA resolution speed
❗ Same ICU stay
❗ Same mortality
➡️ So endpoints look “equal”…
…but physiology is not.
🚨 Why this matters in real ICU practice
Hyperchloremia is not benign:
• Worsens metabolic acidosis
• Increases respiratory workload
• Promotes renal vasoconstriction
• Delays recovery
And hypokalemia?
• Arrhythmias
• Insulin resistance
• Delayed metabolic correction
🧬 Clinical interpretation
This is not about:
❌ “Which fluid resolves DKA faster?”
This is about:
➡️ Which fluid creates a better internal environment for recovery
🔥 Take-home message
👉 NS is acceptable
👉 RL is physiologically smarter
➡️ Especially in:
• Severe acidosis
• High chloride states
• Patients at risk of hypokalemia
📚 Trifi A. et al. (2025)
Medicina Intensiva
doi.org/10.1016/j.medi…
⚠️ Vasopressor weaning in septic shock: the blind spot in current guidelines
We talk a lot about starting vasopressors.
We rarely talk about how to stop them safely.
And that may be a problem.
📌 The gap
The 2026 Surviving Sepsis Campaign provides:
✔️ Clear guidance on initiation
✔️ Clear escalation strategies
❌ But no guidance on de-escalation
👉 Yet this is one of the most frequent bedside challenges
🧠 Key clinical dilemma
Which should be stopped first?
• Norepinephrine?
• Vasopressin?
The answer is… unclear.
📊 Conflicting evidence
👉 Observational studies:
• Higher hypotension when vasopressin is stopped first
👉 Randomized trials (DOVSS, RENOVA):
• Higher hypotension when norepinephrine is stopped first
➡️ Completely opposite conclusions
💡 Why this contradiction exists
It’s not just what you stop.
It’s how you stop it.
👉 Abrupt discontinuation vs titrated reduction
✔️ Most RCTs used protocolized titration
❌ Observational studies often used abrupt withdrawal
➡️ Method matters as much as sequence
🧬 Physiology you should not ignore
• Endogenous vasopressin rises early
• Then drops within ~48h
➡️ Leading to relative vasopressin deficiency
👉 Removing vasopressin at this point may trigger hypotension
🧪 Potential future tool
👉 Copeptin (vasopressin surrogate)
• May predict hypotension after withdrawal
• Not yet ready for routine decision-making
🚨 Clinical reality
There is:
❌ No standardized weaning protocol
❌ No strong guideline recommendation
❌ Limited RCT evidence
But:
👉 This is a daily ICU decision
🔥 Take-home message
Vasopressor weaning is not a passive step.
It is an active hemodynamic intervention.
And currently:
👉 We are navigating it with incomplete evidence
📚 Mallmann C. et al. (2026)
Intensive Care Medicine
doi.org/10.1007/s00134…
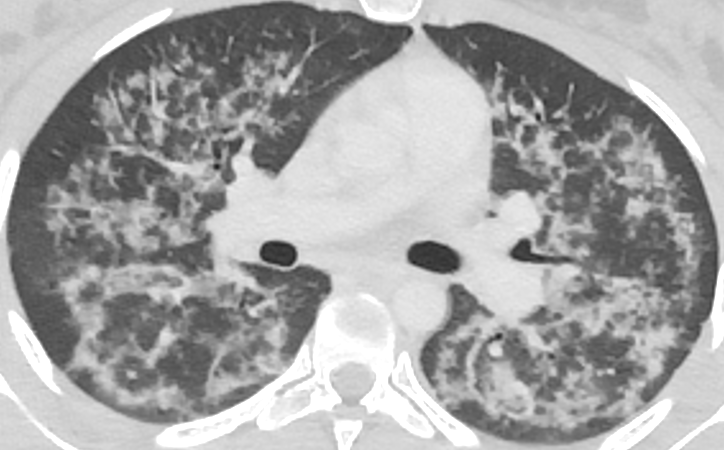
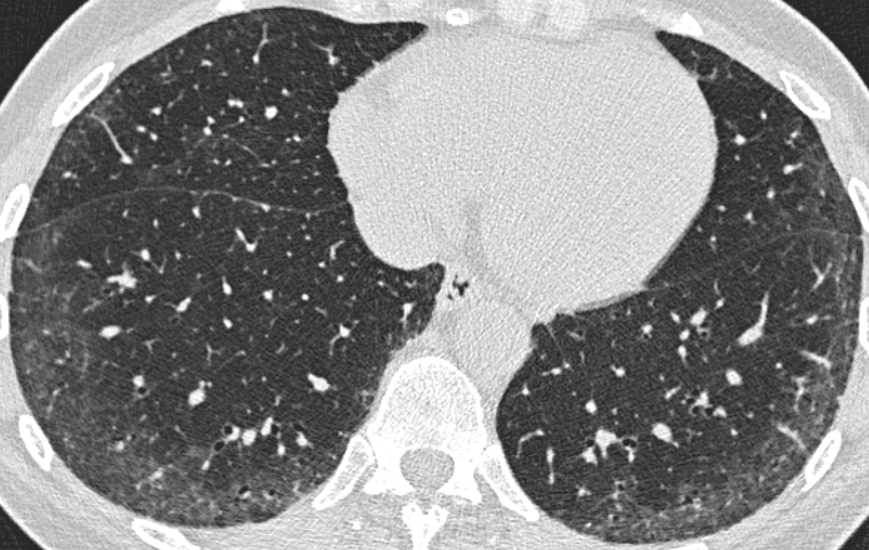
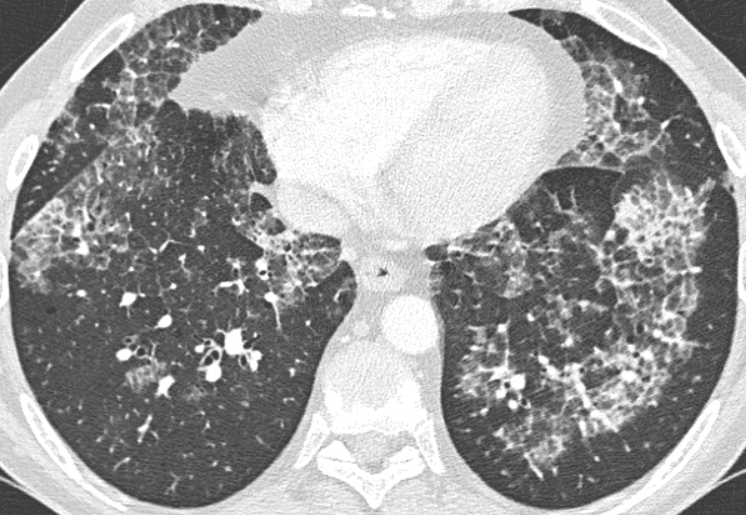
🧵 When you see a "carpet of cysts" on HRCT don't just call it UIP and move on...
That macrocystic honeycombing pattern might be telling you something bigger. 👇
Pooja B sharma as Draupadi is Devine 🪷💯
No one can beat it
One of the best performances in ITV
Namit Malhotra sir should have considered her for the role of Urmila.. dearest sister of maa Sita
#Ramayan@malhotra_namit