Avi Roy@agingroy
14 clinical trial arms. Three pharma companies. Three separate mechanisms. One question. Can you lose weight on Ozempic or Mounjaro without losing muscle?
Lose a kilogram on semaglutide (Ozempic) alone and roughly a third of it is muscle. On tirzepatide (Mounjaro), about 30%. This has been the cost of every obesity drug, diet, and bariatric surgery for decades. Your body doesn't spare muscle during a caloric deficit.
@Regeneron went after myostatin directly. Their antibody trevogrumab, combined with semaglutide in the COURAGE trial (999 patients, 26 weeks), shifted the fat share of weight loss from 67% to 83%. Adding garetosmab, which blocks activin A, pushed it to 92.6%. That three-drug combo lost more total weight than semaglutide alone, and nearly all of it was fat.
@ScholarRock took a narrower path. Apitegromab blocks only the latent form of myostatin. Combined with tirzepatide in EMBRAZE (87 patients, 24 weeks), fat share went from 70% to 85%.
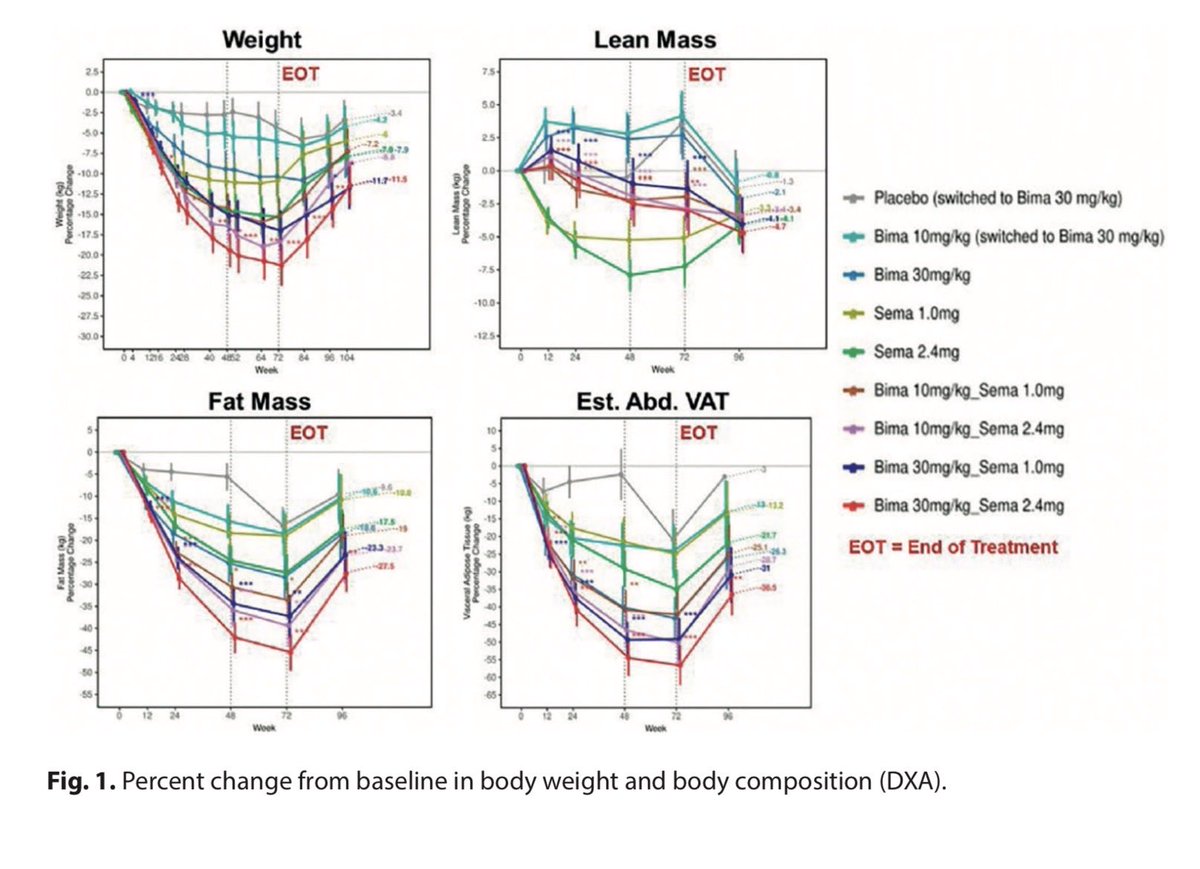
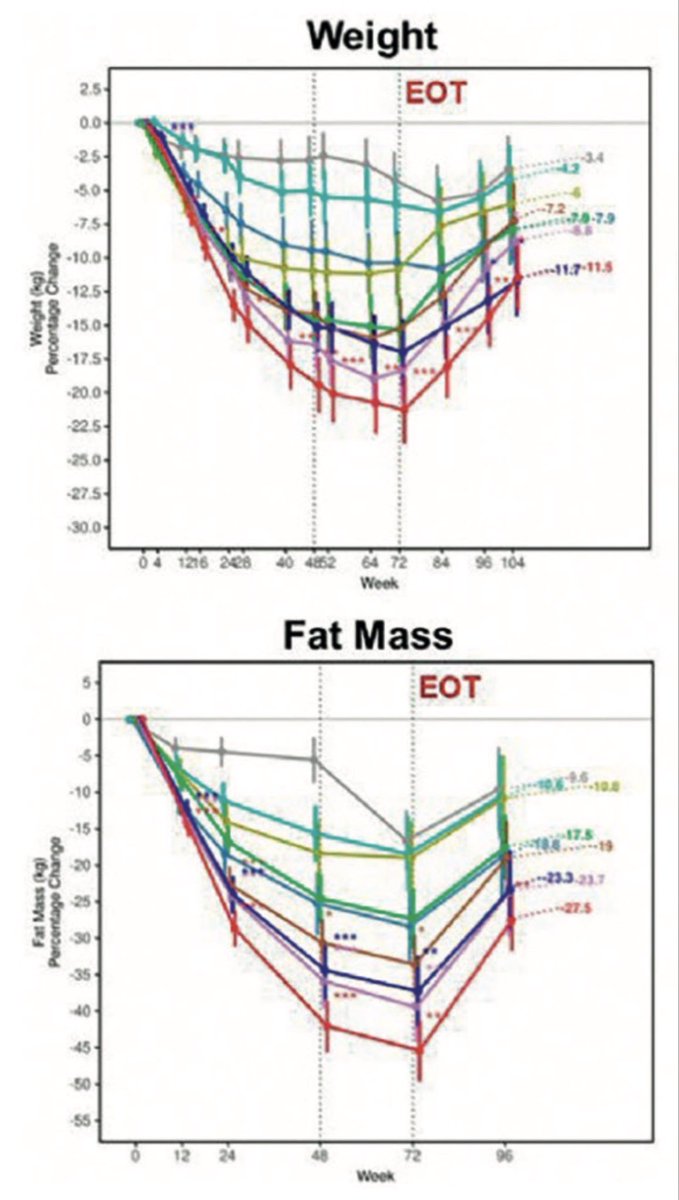
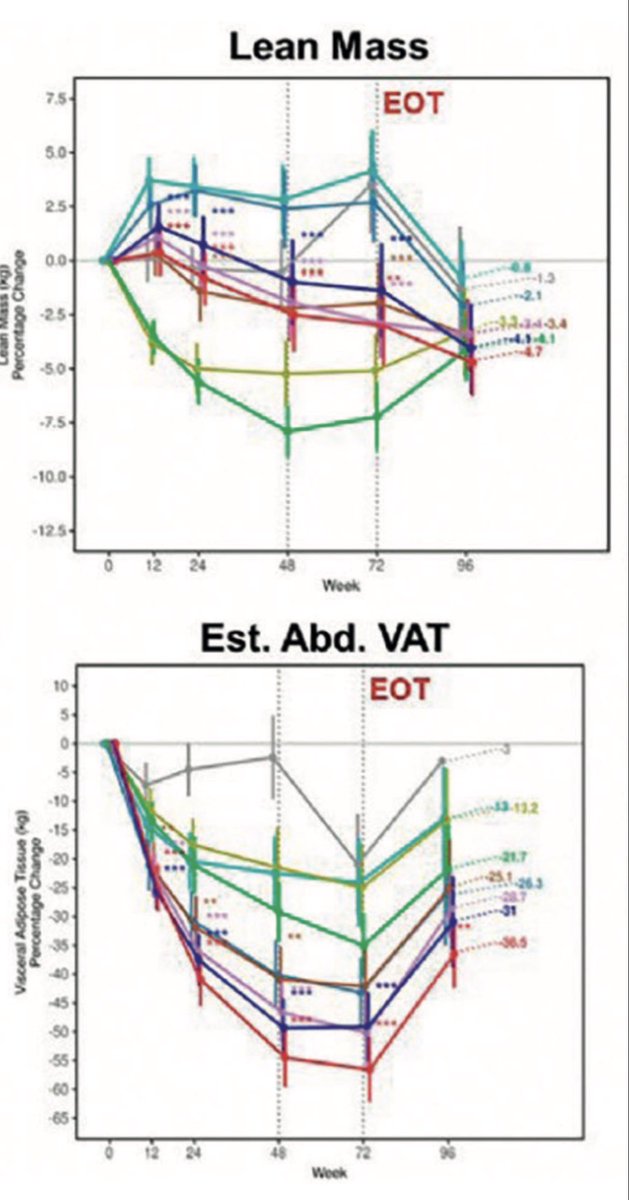
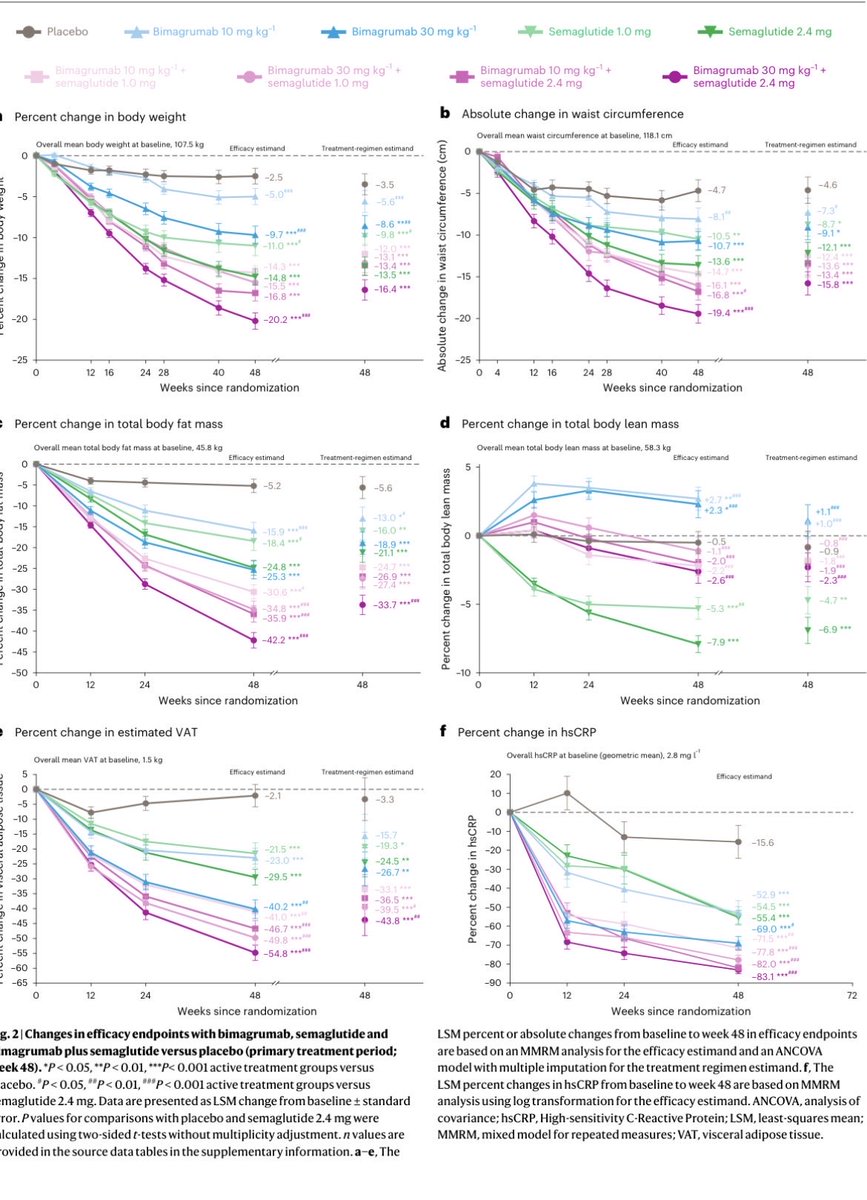
@EliLillyandCo's bimagrumab is the broadest weapon. It blocks the receptor that both myostatin and activin A signal through. In the BELIEVE trial (507 patients, 48 weeks, @NatureMedicine 2026), 92.9% of weight lost with semaglutide was fat. And as a single drug, bimagrumab did something no obesity therapy has ever done. Patients lost weight while gaining 2.5% lean mass. Every gram of weight lost was fat.
The range across all 14 arms runs 67% to 100% fat. Every combination beat every GLP-1 alone. Didn't matter which antibody, which GLP-1, or which company ran the study.
The safety questions are OK. COURAGE's three-drug combo had a 28% dropout rate and 2 deaths. Bimagrumab triggers muscle spasms in many patients. Apitegromab looked cleanest but had the smallest trial.
More than 11 million Americans are on a GLP-1 right now. Most of them are losing muscle they'll struggle to rebuild, especially over 50. These drugs don't just shrink you. They decide what kind of weight you lose.