Sabitlenmiş Tweet

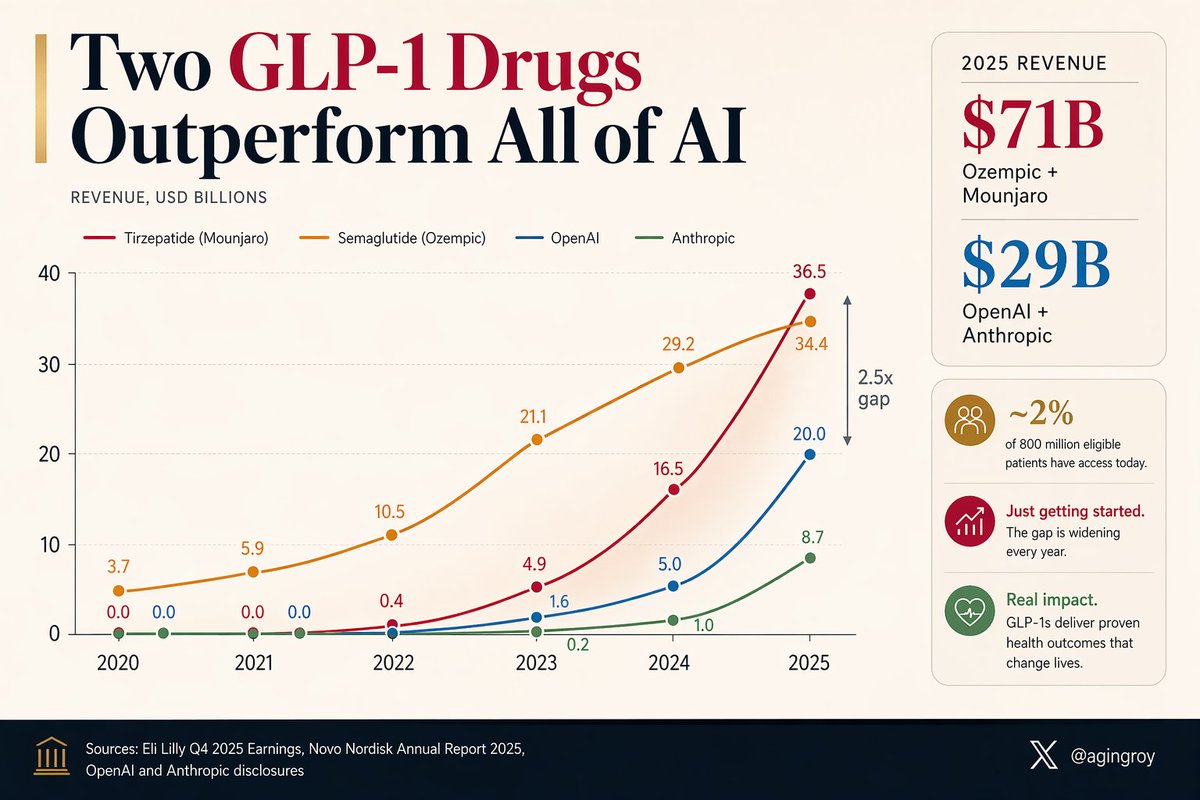
A weekly jab in the belly is generating more revenue than the entire AI industry.
Ozempic + Mounjaro: $71B in 2025.
OpenAI + Anthropic: $29B.
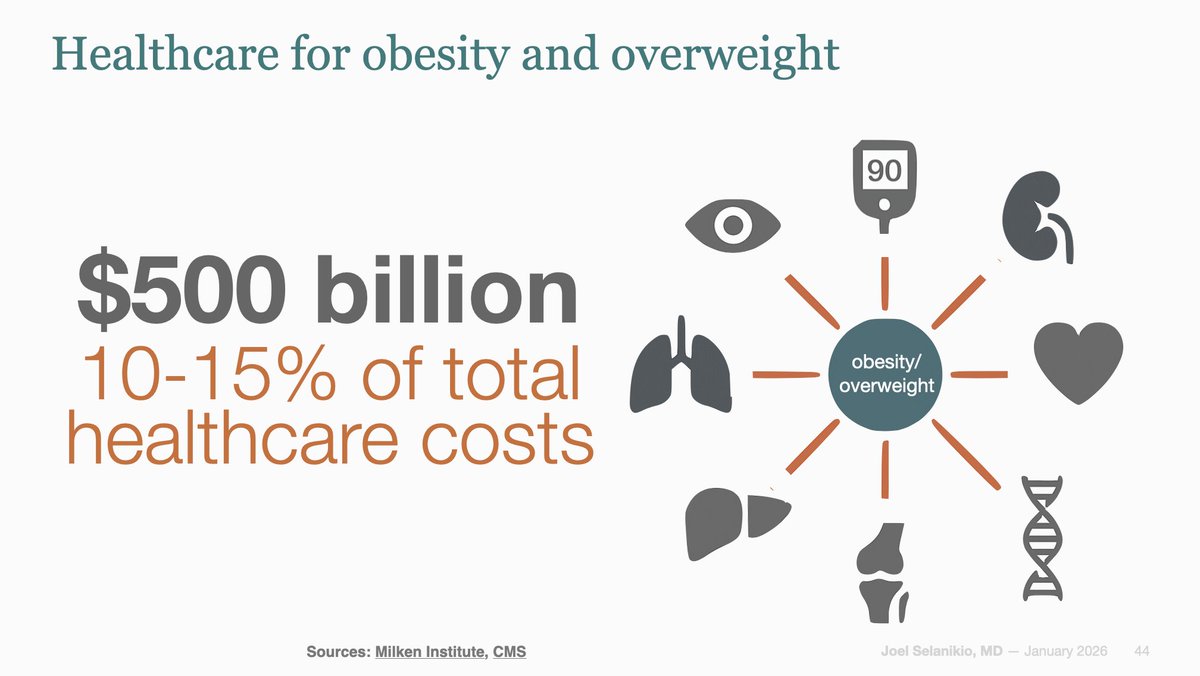
And they've barely started. ~2% of the 800 million eligible patients can currently access them.
h/t @DrSamuelBHume
English