Daniel Portik
1.6K posts

Daniel Portik
@PortikDaniel
Radiation Oncologist | RTQA Fellow @EORTC | SF&Fantasy Reader | Google Reviews Writer | Wannabe Meme Artist



Quick run down of the features on Endpoint Arena, the prediction market for clinical trials. the home page has all the trials:



📗 Just published in the @RO_GreenJournal: ESTRO technical #guideline: intensity modulated radiotherapy and image guided radiotherapy for #rectalcancer 👉 Read the abstract: bit.ly/4axUBK1 #IMRT #IGRT


Update on European Citizens’ Initiatives: 🔹 “Stop Destroying Videogames” has reached the required threshold and is now under Commission examination 🔹 Explore all officially registered initiatives, including the newest one from this week. More: link.europa.eu/PC8mbQ

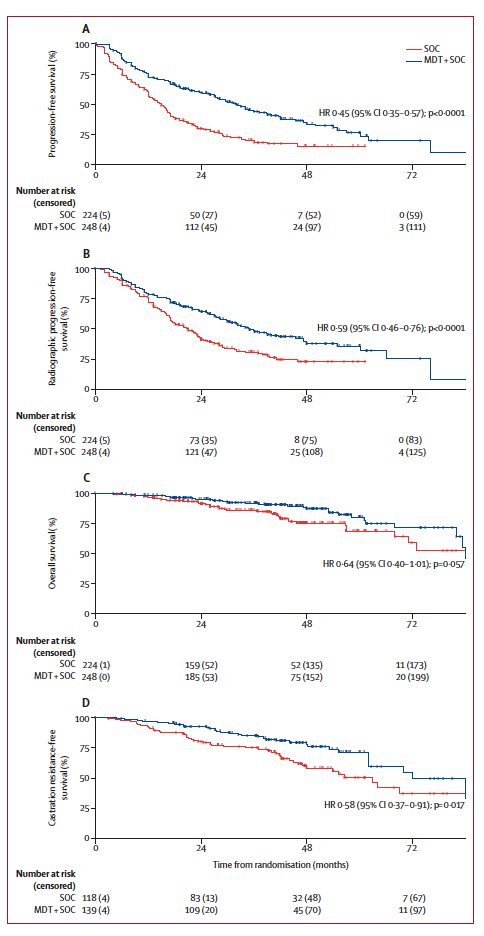
High-Dose Versus Standard-Dose Twice-Daily Thoracic Radiotherapy in SCLC: Final data: Median OS in the 60 Gy group was significantly longer (43.5 versus 22.5 mo) Same toxicity. jto.org/article/S1556-…




Operable is a clinical label, and doesn't always mean the 'right' choice. The right decision depends on the life a person wants to live after treatment. When treatments are comparable, the decisions must center on what matters most to patients, which is why honest, nuanced, informed conversations are critical. Patient preferences should always guide treatment decisions. #LCSM #LCAM
💥 Ablative Radiation… and Delayed Surgery in Ca Breast? The Rahimi Trial | JAMA Network Open 2025 🔥 💡 Single-fraction preoperative stereotactic partial breast irradiation (sPBI) in early HR+ breast cancer. 30 vs 34 vs 38 Gy - all in ONE shot ⚡️ Endocrine therapy ➜ ⏳ wait ➜ ✂️ delayed surgery. And the results are wild. 🤯 🎯 Trial Essentials • 🧪 Phase 1 | n = 44 • 🎀 HR+, HER2-neg, cN0 • 🎯 sPBI: 30 / 34 / 38 Gy (1 fraction) • 💊 Endocrine therapy after RT • 🗓️ Surgery allowed up to 12 months later 📈 Key Results 1. Safety • 🚫 MTD not reached up to 38 Gy • 😊 Mostly grade 1 • ⚠️ 1 late G3 wound issue (diabetes) 2. Response Rates 30 Gy → pCR 36% | pCR+near pCR 64% 34 Gy → pCR 47% | pCR+near pCR 93% 38 Gy → pCR 67% | pCR+near pCR 93% 💥 If surgery delayed >9 months: • pCR 72% • pCR+near pCR 92% 🧬 Biology Behind It • 📉 Ki-67 dropped 11% → 2% • 🟩 95% had Ki-67 <3% in residual disease • 🧲 Radiation + endocrine therapy = slow, sustained tumor kill • ⏳ Time > Dose 🧭 What Mattered Most? Time to surgery • 📈 Strongest predictor of pCR • ➕ Each extra day improved odds • 🎚️ Dose beyond 30 Gy gave minimal extra benefit • 🕘 Surgery >9 months = best response ✨ Takeaway A single 30–38 Gy shot ⚡️ + endocrine therapy + delayed surgery might be the first step toward no-surgery management for select early HR+ breast cancers. 🚀 Opens the door for true “radiation-only” curative trials.” 💡 Future paradigm: Ablate 🔥 • Wait ⏳ • Omit Surgery ✂️ …for carefully selected luminal A disease. 📓Full paper in comment below ⬇️ #BreastCancer #RadiationOncology #MedTwitter #OncoTwitter @JAMANetworkOpen @myesmo @esmo_open @ASCO @OncoAlert