Richard Anderson retweetledi

Castell Harlech has watched over this landscape for 700+ years. Built by Edward I, it has endured rebellion, siege and shifting tides—now overlooking Royal St David’s, where the game unfolds beneath its shadow.




English
Richard Anderson
4.2K posts


@RAAnderson1
Father, Professor, Interventional Cardiologist, researcher, free thinker, athlete possibly




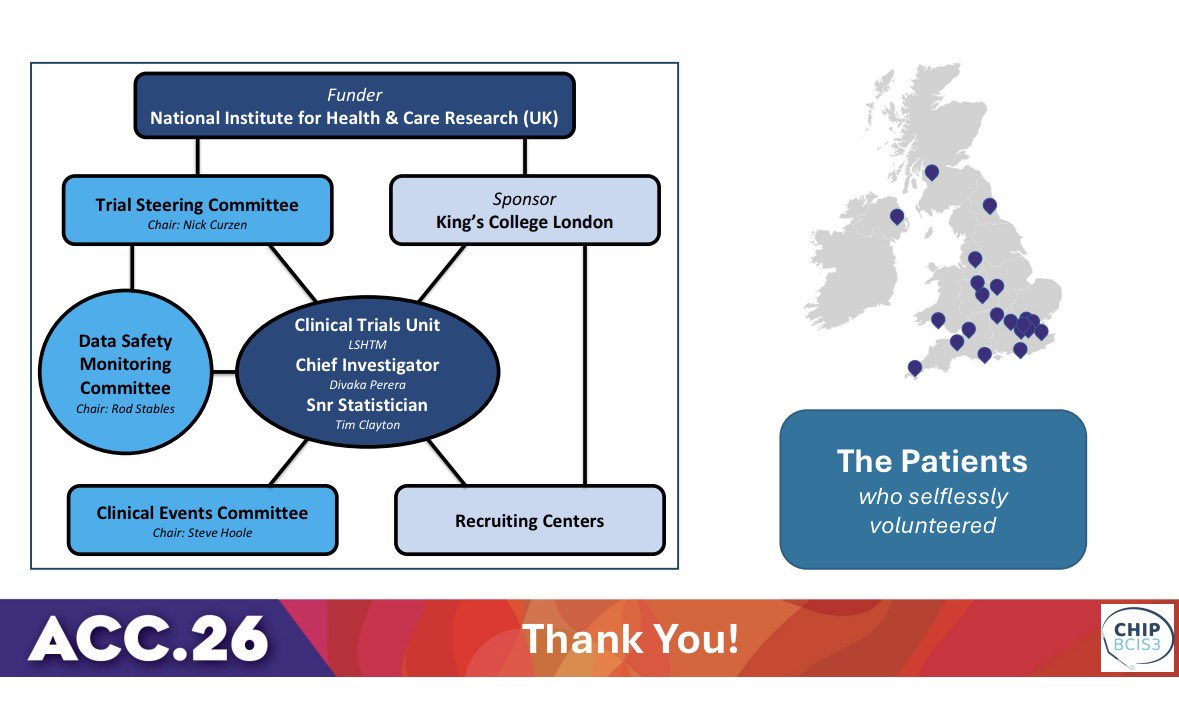

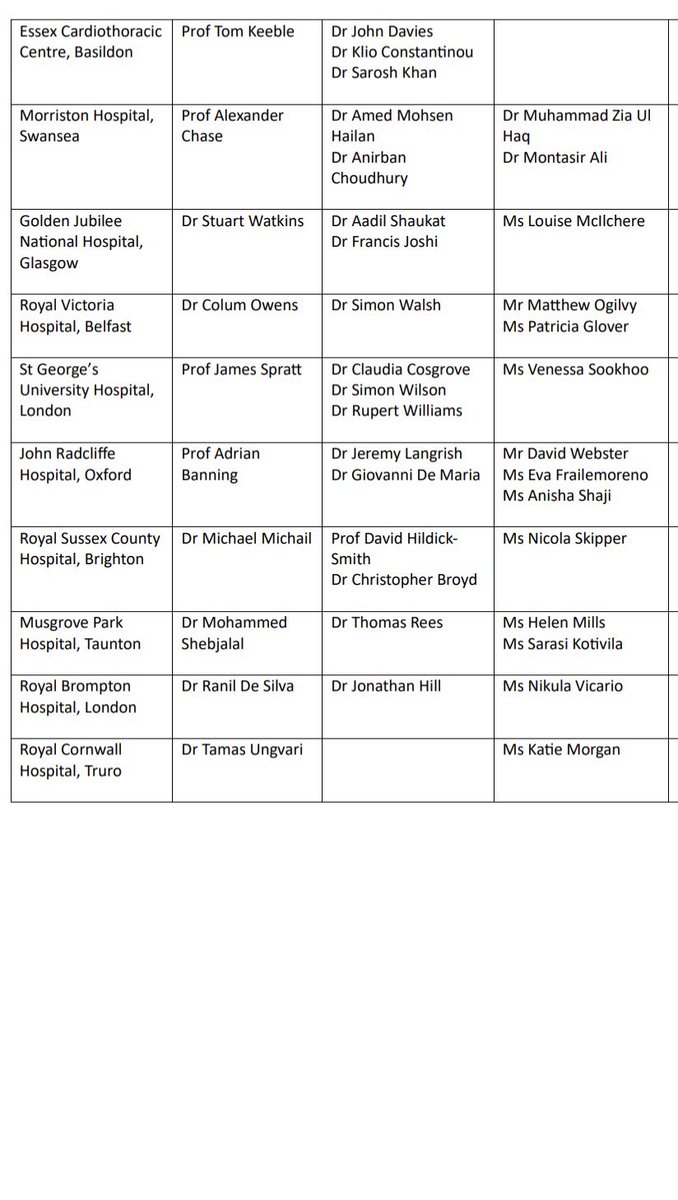











🚨 CHIP-BCIS3 randomised 300 patients with LVEF ≤35% undergoing high risk PCI to either micro axial flow pump or standard care ➡️ mAFP did not reduce major adverse clinical outcomes ⚠️ There was an excess of CV death in patients who received PCI with mAFP #ACC26 @BCIS_uk

#acc26 Six reasons why CHAMPION AF should not change oral anticoagulation for AF I will have a formal post up on @theheartorg but here is a short summary 1) Stroke and Ischemic Stroke went the wrong way. All S -> 33 vs 50 [HR 1.46 95% CI, 0.94-2.27)] IS -> 27 vs 45; [HR = 1.61; 95% CI, 1.00-2.59)] Look at those upper-bounds. 2) NI would not have been met for efficacy had they used a margin with both rate ratio and risk difference, which is standard practice. The margin of 4.8% is based on event rates at 12%, which is 1.4 in relative terms (40% higher). But when event rates come in lower, as they did: 4.8% vs 5.7%, the 4.8% margin is too lenient. The 0.9% higher rate of the primary endpoint has a 95% CI of (-0.8-2.6%), so 2.6% is less than the margin of 4.8%. Now do it with relative risk. It's in table 2. The relative risk is 1.20. The 95% confidence intervals were 0.87-1.66. Note that 1.66> 1.40 so LAAC is not noninferior based on rate ratio margins 3) The primary safety endpoint is flawed because it excludes periprocedural bleeding and uses nonmajor bleeds, such as gum bleeds and bruising. It's open label trial so who which group will complain of more nonmajor bleeding? 4) When counting all events, Watchman barely reduced major bleeds. Also in the main results table is that major bleeds were 83 vs 87 (5.5% vs 5.8%; HR 0.92 95% CI 0.68-1.24) 5) Net Clinical Benefit was also flawed because they used nonprocedural bleeding and nonmajor bleeds. A normal patient would simply say, there were 17 more strokes and only 4 less bleeds. Hardly a good trade. 6) Bayes: trials don't give answers, they update priors. For Watchman, you have PREVAIL failing against warfarin, CLOSURE AF clearly failing against best med Rx (mostly DOACs) so priors are pessimistic. To go from pessimistic priors to enthusiastic posteriors you'd need hugely positive data. CHAMPION is not that. Don't believe the stories that CLOSURE failed due to them using other LAAC devices. In the AMULET IDE trial, Watchman and Amulet were similar. Also, if you believe that German operators are worse than US authors, you need to travel more. Conclusion: Oral anticoagulation for AF is one of the most evidence-based practices in all of medicine. To upend that would take much stronger data. Don't be bamboozled by this trial, which was designed to be positive before the first patient was enrolled. #ACC2026

@BSCMR @BSHeartFailure @BHRSociety @BritishCardioSo endorsement of the BRITISH RCT. 1252 patients with NICM scar and ef<35%. ICD Vs no ICD. All cause mortality. Over 550 patients recruited. Australian sites opening in March. @TheBHF @SouthamptonCTU @ncurzen @josephselvanay2
How should we guide selection of invasive therapies following an out-of-hospital cardiac arrest? Prospective validation of the MIRACLE2 Score @ncurzen @krishnaraj82 @garryhamilton6 @drR_Simpson @Sam_mc35 @zaidiskandar85 @DrPaulRees ahajrnls.org/4saBexX



Voting for Members and Fellows opens today in the @RCPhysicians election. I'm standing for council and would appreciate your support so we can tackle the issues facing doctors and the RCP @mmamas1973 @Azeem_Majeed @drtkeebl @cpgale3 @goldstone_tony @DrDerekConnolly @ProfDerekBell @mancunianmedic @doctor_oxford @scserendipity1