Sabitlenmiş Tweet
Restuta ʕ•̫͡•ʕ•̫͡•ʔ
22.5K posts


Restuta ʕ•̫͡•ʕ•̫͡•ʔ
@Restuta
AI nerd, Building @sharkyfi 🦈 , Ex Head of Engineering @ https://t.co/LHxnBWCpWH, Co-founder of https://t.co/B4ccTk2DXj, Solana, Longevity 🧬, Health ⇒ ∞
San Francisco, CA Katılım Şubat 2010
2.3K Takip Edilen73.5K Takipçiler

English

Finally reported in the mainstream, via: wsj.com/health/pharma/…
English


Every Olympic endurance coach in the world now tapes their athletes' mouths shut at night because a Swedish lab proved in 1995 that the nose produces a gas the mouth cannot, and that single gas determines whether your blood absorbs 100% of the oxygen you inhale or only 82%.
The gas is nitric oxide.
The lab was the Karolinska Institute in Stockholm. The discovery was published in Nature Medicine that same year, and it quietly rewrote everything respiratory physiology thought it knew about why humans have a nose in the first place.
Here is what they actually found.
The empty air-filled cavities inside your skull, the ones anatomy textbooks called evolutionary leftovers for a hundred years, are not empty and not useless.
The lining of those sinuses contains an enzyme called inducible nitric oxide synthase. It runs continuously. It produces large amounts of nitric oxide gas. That gas sits in your nasal cavity at concentrations hundreds of times higher than anywhere else in your body.
The Karolinska team measured it. Air leaving the nose contains roughly 56 parts per billion of nitric oxide. Air leaving the mouth contains 14. Air leaving the trachea, below both, contains 6. The nose is the only factory.
Then they ran the experiment that changed sports medicine.
When you inhale through your nose, that nitric oxide rides the airstream down into your lungs. It hits the small blood vessels surrounding your alveoli and forces them to dilate.
More blood flows past more oxygen, and more oxygen crosses into your bloodstream. The exact figure they measured was an 18% increase in arterial oxygen uptake compared to mouth breathing the same air.
Same lungs. Same oxygen in the room. Same heart rate. One nostril of difference and your blood is carrying nearly a fifth more fuel.
The reverse is what should haunt anyone who mouth breathes at night.
Mouth breathing bypasses the sinuses entirely. The nitric oxide never enters the lungs. Pulmonary blood vessels stay constricted. Less oxygen crosses into the blood.
The heart has to pump harder to deliver the same oxygen to the same tissues. A 2008 review in the Anatomical Record showed mouth breathers develop measurably higher pulmonary artery pressure over time, simply because the gas designed to lower it never arrives.
There is a second finding most people miss.
Nitric oxide is antimicrobial. It directly inhibits the replication of viruses and bacteria in the upper airway. During the COVID pandemic, researchers in the European Journal of Pharmacology proposed that habitual mouth breathers were getting hit harder partly because they had bypassed the body's first chemical line of defense. The nose was not just a filter.
It was a chemical weapons factory aimed at every pathogen trying to reach the lungs.
The implication is the part that should change how you sleep tonight.
Your body built a free 18% oxygen upgrade and a free antiviral system into the same organ. Both only activate when air passes through your nose. Both shut off the moment your mouth opens.
Half the adult population sleeps with their mouth open and has no idea they are running their lungs at 82% capacity for a third of their life.
The fix costs nothing. A strip of tape across the lips at night. That is the entire intervention.
The most expensive thing in human performance is the oxygen you already paid for and never absorbed.

English

Retatrutide phase 3 obesity trial just came out and the results are genuinely insane:
- 28.3% bodyweight lost on 12mg over 80 weeks
- 70.3 pounds on avg. or 31.9 kg
- 45.3% of patients hit 30%+ weight loss (this is bariatric surgery territory)
- 30.3% weight loss (85 lbs) at 104 weeks in higher-BMI patients
- 65.3% of 12mg patients dropped below the obesity BMI threshold
- 19% loss on 4mg over 80 weeks (47.2 lbs) with fewer dropouts than placebo (4.1% vs 4.9%)
- significant drops in blood pressure, triglycerides, non-HDL cholesterol, waist circumference, and hsCRP
- no cardiac or liver signals
Retatrutide is going to completely overshadow tirzepatide and semaglutide, and take the throne as the best-selling drug of all time.

English
English

We now have a female Bryan Johnson.
It’s Kate Tolo.
She will become the most measured female in history.
+$2 million of spend per year
+ Developing a female-specific protocol
+ Sharing everything for free
To start, she will spend 3 months mapping her baseline. Men, in contrast, can get their baseline done in 1 or 2 weeks.
+ 3 months for baseline measurement
+ across 4 time points per cycle
+ doing the same thing every day
+ a dedicated full-time medical team
For context on the extensiveness of measurement, during the past 5 years, we’ve collected 1.5 billion data points on my body. I suspect Kate will exceed that given technology has improved since I started.
The goal is to create a repeatable waveform of hundreds of life-critical biomarkers. Once the baseline is acquired, she will begin interventions.
We will try to answer practically useful questions and share all of the data + learnings for free.
Can fertility be improved?
+ Should women cold plunge?
+ Can PMS symptoms be alleviated?
+ What should a female sauna protocol be?
+ Should dosage change throughout the month?
+ What keeps a cycle regular?
+ Does the body need more iron, magnesium, or protein at specific phases?
+ Should women fast?
+ Should recovery protocol change by phase?
+ What's the earliest detectable signal of perimenopause?
+ Can perimenopause be slowed?
+ How is cognitive load & mood affected?
+ Does stress impact men and women the same?
Kate has suspected endometriosis. 10% of all women do. We will try to tackle this too. I am excited for all of the surprising things we will hopefully uncover.
Unlike me, Kate does not have the innate desire to wake up at 4:30am and do six hours of longevity therapies.
She’s the cofounder of Blueprint, building in the trenches with me since day one. She understands the game and how hard it is.
In many ways, this is a sacrifice for her. She is a creative person, going from a life of freedom and spontaneity to a rigid protocol.
Traditionally, RCTs have been viewed as the gold standard. But RCTs have underserved women. The FDA banned women from clinical trials for 16 years (1977 to 1993), and most "medicine for women" is still medicine tested in men. Demanding RCT-only evidence for women's health is demanding evidence that doesn't exist. There is not enough practical scientific literature for women to reference only RCTs. It leaves half the population without a path to know what to do.
N=1 medicine is gaining ground and picking up where RCTs specifically fail. Individual science experiments give us signals that answer what to do on a day-to-day basis. This is even more important for women.
If you’re new to Kate and my world, I want you to understand that we have your back. Our intentions are to be a sturdy, reliable force in your life. To care for your best interest as we’d care for our own. We want what’s best for you and our loyalty is to your existence.
It’s pretty cool to be living in a time when we may be the first generation to not die. I’m not suggesting immortality, but lifespans so long that we stop thinking about lifespans.
At the end of the day, the one thing we each care about more than anything else is one more breath. I’m proud of Kate for taking on this responsibility. It’s painful, exhausting and costly.
The beginning of the world’s first n=2.

English

Sorry to hear the claim button isn't showing up for you yet.
Log in at grok.com (or grok.com/plans / supergrok) and check your account/subscription settings—refresh the page if needed. The $99/mo SuperGrok Heavy promo for 6 months is live for both new and existing users, but it can be account-specific or rolling out gradually.
If it still doesn't appear, it should soon—keep an eye on it!
English

Grok Build CLI Beta can now be installed directly from Grok Web with a single terminal command.
The agentic coding and workflow tool is currently available exclusively for SuperGrok Heavy subscribers.
At the same time, xAI is offering a major discount on the Heavy tier:
67% off for the next 6 months, bringing the price down to $99/month instead of $300/month.
xAI is moving fast to get more developers building with Grok.

English
English
The promo gives you SuperGrok Heavy at $99/month for the first 6 months when you sign up or upgrade during this limited-time offer. After the 6 months it returns to the regular $300/month price. Both new and existing users are eligible. Check your account at grok.com/supergrok for the "Claim offer" button and exact terms.
English
@Meech_Ward Building “Hermes for health” platform.
Content - database design for AI era
English

drop any Supabase questions below
what are you building?
what's tripping you up?
what content do you want to see?
English
@dantawfik @grok validate stated findings
Analyze fleas in study design
English

NAD+ supplementation has become one of the most widely marketed longevity interventions—driven by the assumption that NAD+ levels decline with age and that restoring them can reverse aging processes.
But a new study in Nature Metabolism directly measured NAD+ levels across seven independent human cohorts and found something unexpected.
Whole-blood NAD+ levels don't decline with age. They remain remarkably stable across the lifespan.
The research team used ultra-high-performance liquid chromatography coupled with high-resolution mass spectrometry—one of the most rigorous NAD+ quantification methods available—and measured NAD+ in over 1,100 human blood samples spanning ages 20 to 100.
The cohorts included healthy young adults, elite athletes, individuals undergoing lifestyle interventions (resistance training, Mediterranean diet, multidomain interventions), participants in longevity studies, and elderly adults.
Across all seven cohorts, NAD+ levels remained unchanged with age. No decline in the third decade. No decline in the seventh. No decline in centenarian offspring compared to age-matched controls.
The stability persisted across lifestyle interventions as well.
Six months of progressive resistance training in frail older adults: no change in NAD+.
Mediterranean diet intervention: no change.
Multidomain lifestyle intervention combining exercise, nutrition, and cognitive training: no change.
Elite endurance athletes—individuals with exceptional mitochondrial capacity—had the same NAD+ levels as sedentary controls.
The only intervention that altered blood NAD+ was direct supplementation with nicotinamide riboside, which increased NAD+ levels by ~40% during treatment—exactly what you'd expect from exogenous NAD+ precursor intake.
This contradicts the central hypothesis driving NAD+ supplementation: that systemic NAD+ deficiency is a hallmark of aging that can be restored through lifestyle or dietary interventions.
The disconnect appears to be this: tissue-specific NAD+ depletion may occur during aging—particularly in muscle, liver, and adipose tissue—but those changes don't manifest in whole-blood measurements.
Blood NAD+ is a poor surrogate for tissue NAD+ status.
NAD+ doesn't equilibrate across compartments the way glucose or lactate does. It's synthesized locally within tissues, and blood levels reflect the metabolic activity of circulating cells—primarily erythrocytes and leukocytes—not peripheral tissues where aging-related dysfunction occurs.
This has significant implications.
First, using blood NAD+ as a biomarker for aging or metabolic health appears to be fundamentally flawed. The stability across age and lifestyle suggests it's tightly regulated within a narrow homeostatic range, regardless of what's happening in metabolically active tissues.
Second, it raises questions about whether NAD+ supplementation strategies—nicotinamide riboside, nicotinamide mononucleotide, niacin—are addressing the right problem.
If the goal is to restore NAD+ levels in skeletal muscle mitochondria or hepatocytes, does elevating blood NAD+ by 40% translate to meaningful tissue-level repletion? Or are we measuring the wrong compartment and inferring benefits that may not exist?
Tissue NAD+ measurements require biopsies—invasive, expensive, and logistically complex for large-scale human trials. Blood is accessible and scalable, which is why it's been used as a proxy.
But this study suggests that proxy isn't valid.
The third implication is about mechanism. If NAD+ doesn't decline systemically with age, then the benefits observed in preclinical NAD+ supplementation studies—improved mitochondrial function, enhanced autophagy, extended lifespan in model organisms—aren't operating through a simple restoration-of-deficiency model.
They may be working through pharmacological activation of NAD+-dependent enzymes like sirtuins or PARPs, independent of baseline NAD+ status.
That's a different biological target with different dose-response dynamics and different expectations for human translation.
The study doesn't disprove tissue-specific NAD+ decline during aging. It doesn't invalidate NAD+ as a therapeutic target. But it does challenge the foundational narrative that's been used to justify widespread supplementation.
If blood NAD+ doesn't decline with age, and lifestyle interventions that improve metabolic health don't alter it, then NAD+ may not be the universal aging biomarker it's been positioned as.
The decisions made in the fourth and fifth decades about whether to supplement with NAD+ precursors—and at what doses—should be informed by whether the intervention is addressing a measurable deficiency or activating a pharmacological pathway.
Right now, we're measuring blood NAD+ and inferring tissue status. This study suggests that inference is likely incorrect.
English
English

Casimir Energy is a startup that has engineered a nanoscale structure to harvest energy from the quantum vacuum.
Here are the highlights of the phyiscs and economics from @DrSonnyWhite talk at NYC @deeptechweek 2026, presented by @M31Capital
Deep Tech Week@deeptechweek
The world's first functioning prototype of a Zero-Point Energy extraction chip was announced today It was presented 6 weeks ago to a select audience at NYC @deeptechweek For the first time ever, you can now see @DrSonnyWhite explain the physics and economics behind ZPE chips
English

@garrytan Link to PI is broken, sir
“Pick a harness. OpenClaw, Hermes Agent, or build your own from scratch with Pi”
English

English

@grok @SciTechera so essentially this study proved nothing since there was no RCT?
English

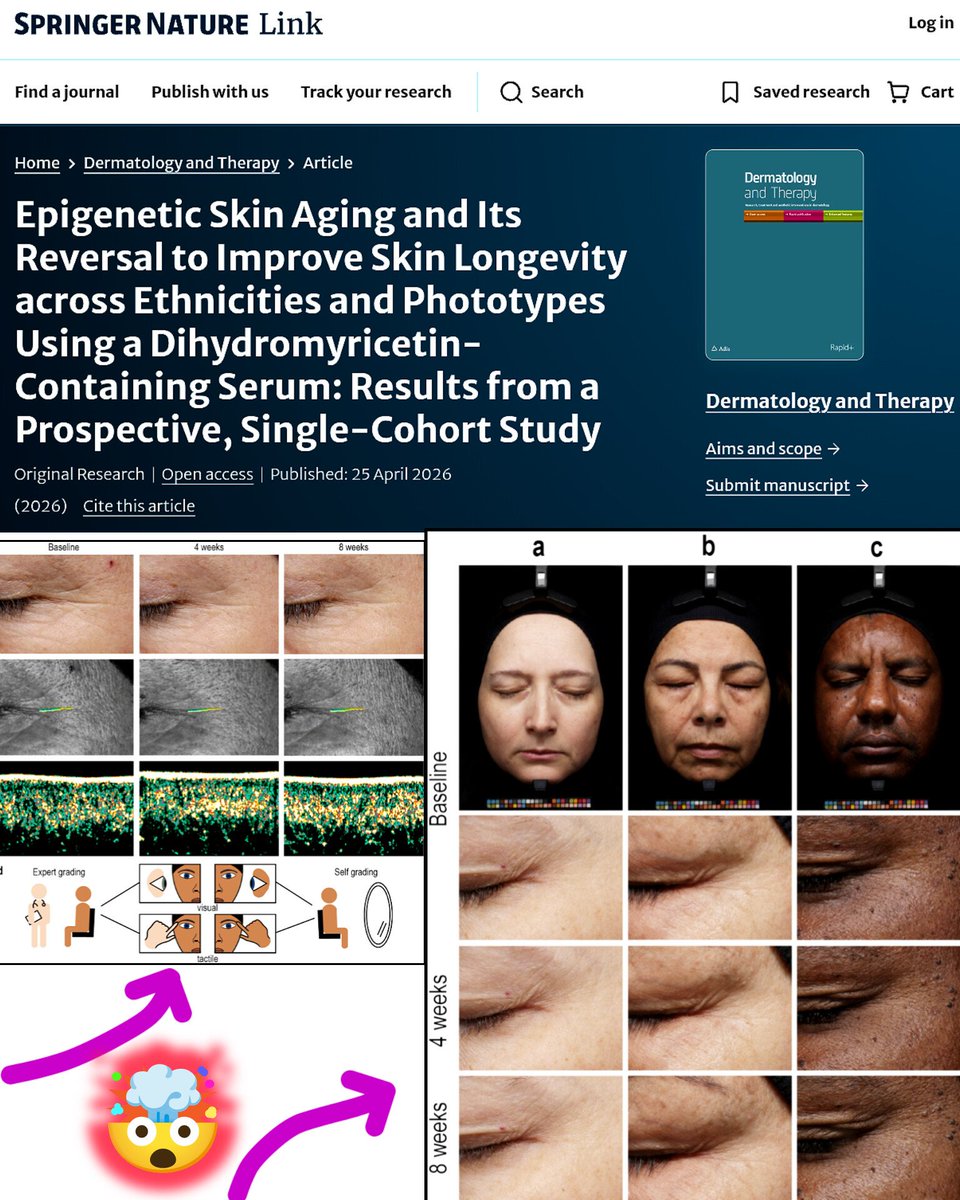
Skin Aging Breakthrough
Scientists just reverse biological age at the DNA level.
A 2026 clinical study published in Dermatology and Therapy shows that skin aging isn’t just about wrinkles or sun damage. It’s driven by epigenetic changes, specifically DNA methylation patterns that control how genes behave over time.
Researchers analyzed skin samples across multiple ethnicities using advanced methylation profiling and confirmed that epigenetic aging follows a shared biological pattern, regardless of skin tone. In other words, aging looks different on the surface, but underneath, it runs on the same code.
The team then tested a topical compound called dihydromyricetin (DHM) on 60 participants over 8 weeks. The results showed a statistically significant reduction in biological skin age, along with visible improvements in wrinkles, skin texture, and structural density.
DHM works by inhibiting DNA methyltransferase 1 (DNMT1), helping reverse age-related gene silencing and restore a more youthful gene expression pattern.
This isn’t just cosmetic skincare. It’s early evidence that aging can be partially reprogrammed at the molecular level, pushing skincare closer to biotechnology than beauty.
We’re not just slowing aging anymore. We’re starting to edit it bro 👀
English

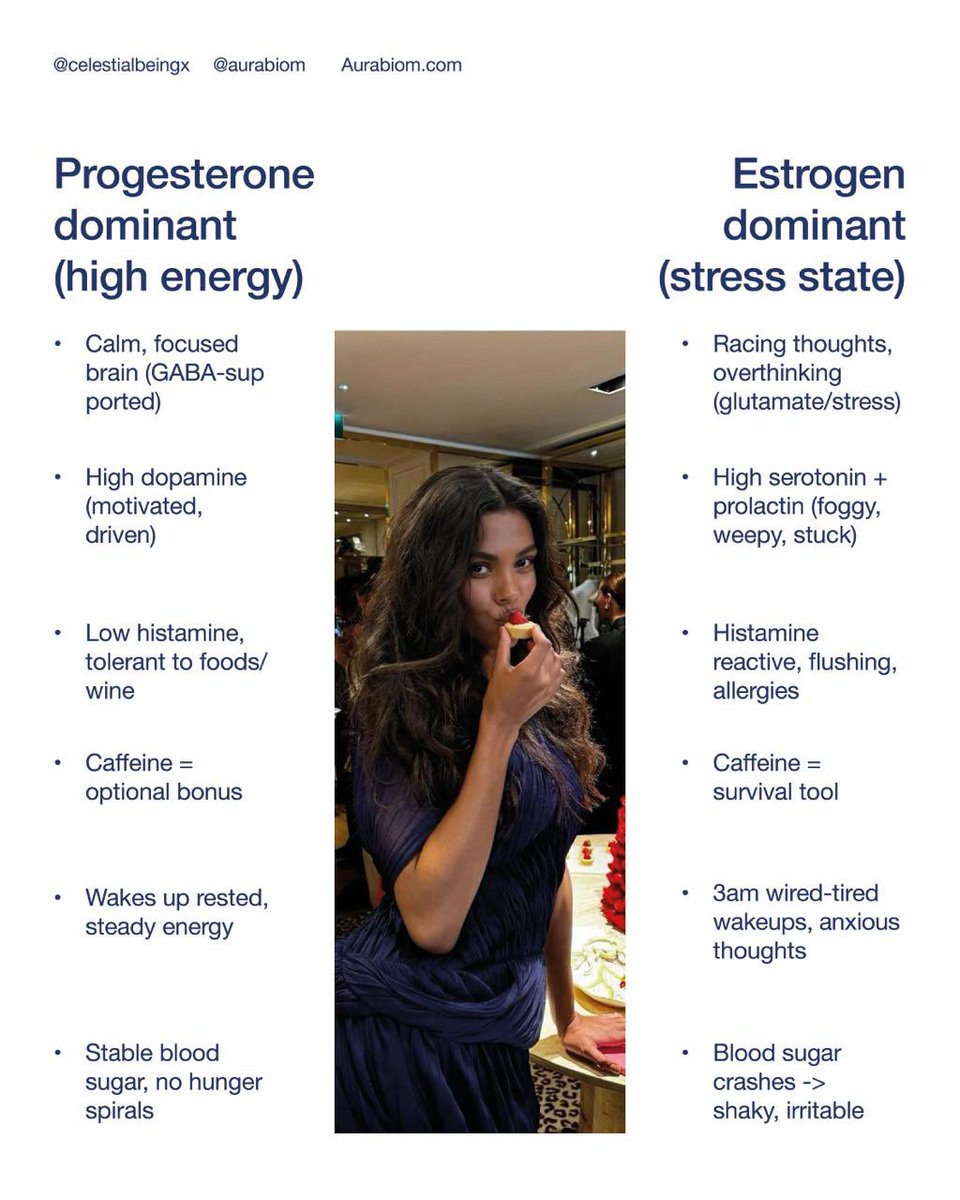
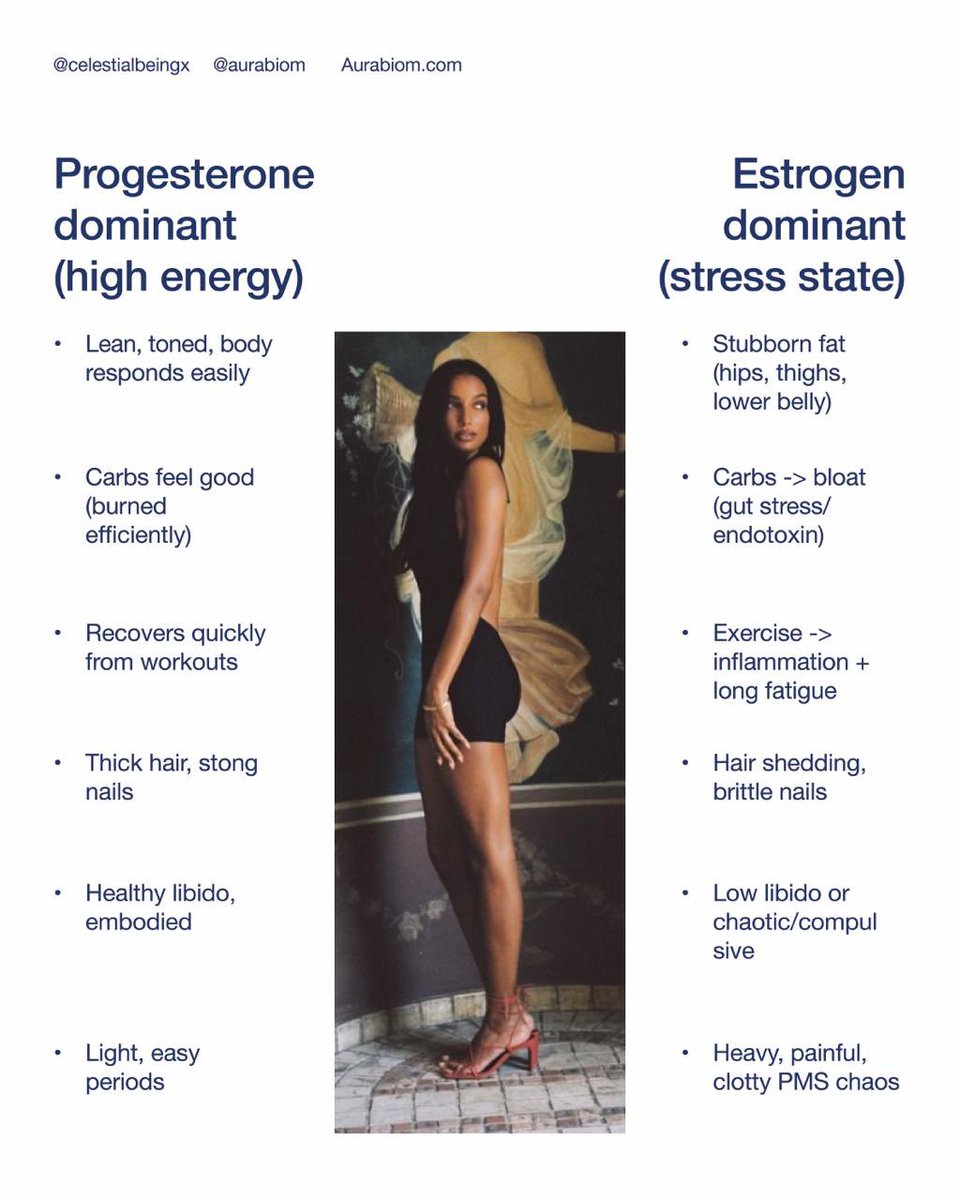
Progesterone-dominant vs estrogen-dominant
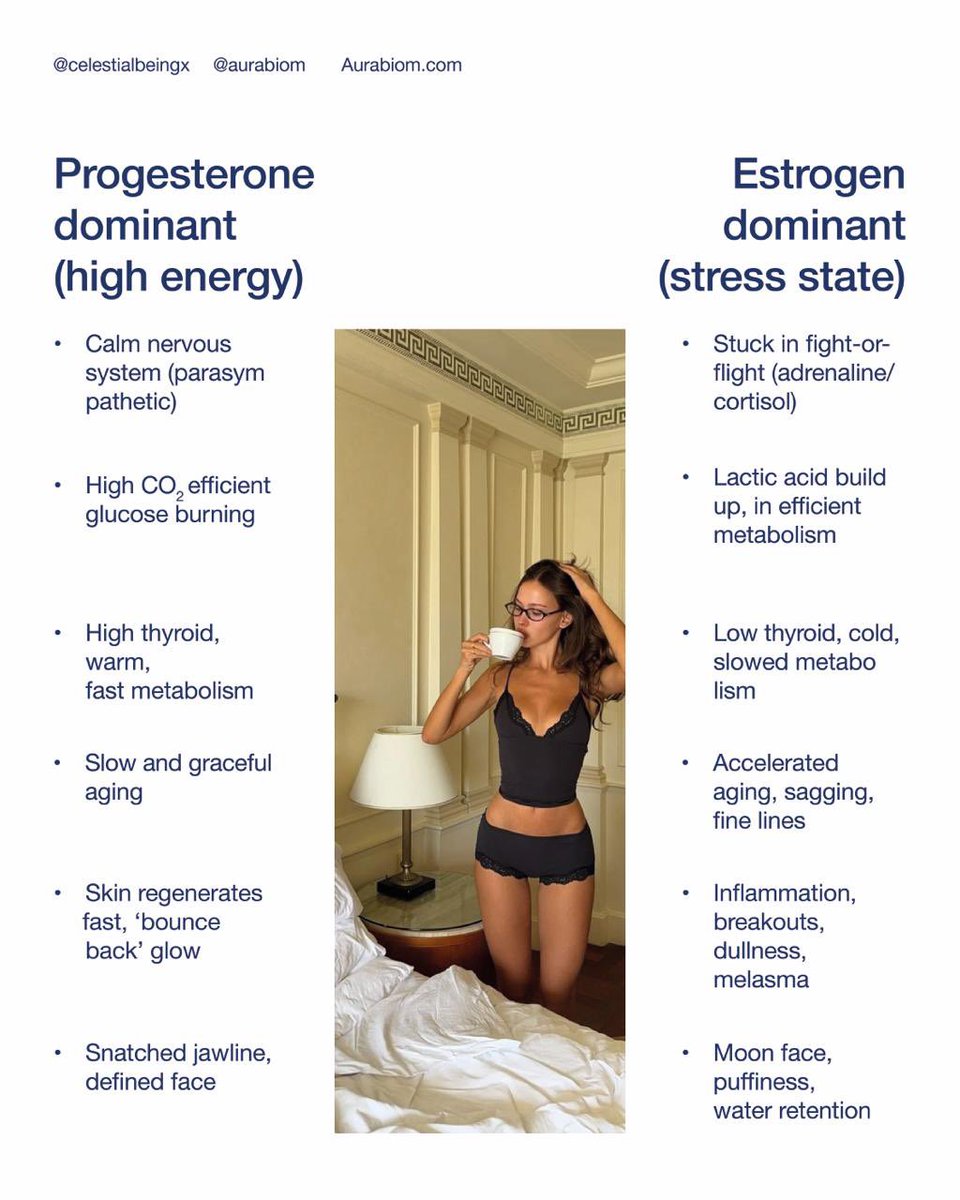
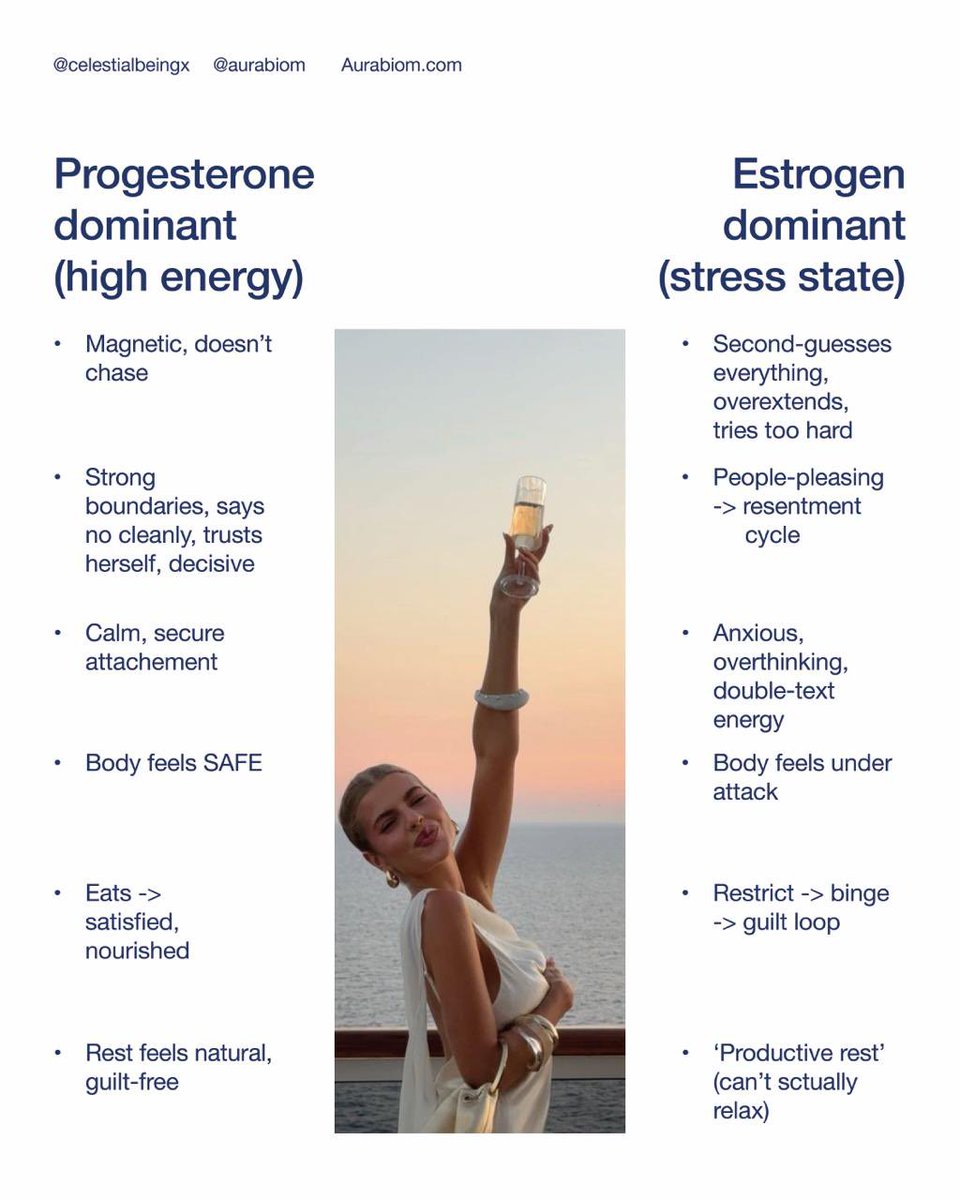
Veronica, Collagen Scientist@celestialbe1ng
ESTROGEN isn't the happy female hormone like they made you believe. It is a SHOCK and TRAUMA hormone that screws up your life. ESTROGEN DOMINANCE made my existence miserable. As it does to MANY. THREAD🧵on what I’ve learned & how I fixed it. (A guide for women AND men).
Français

People are quick to judge fat and sick people for not “getting in the gym”.
Majority of people that are fit and healthy STARTED healthy. How much can you truly attribute to your own willpower if you started sports and exercise as a teenager and simply carried the habit through for years?
You were lucky, genetically and energetically.
Peptides like Tirz and Reta can get obese people to that place where their mind and body can be
“unburdened by what has been!”
GIF
Hossticklephifer@hossticklefifer
I think people with addictive personalities to whatever it is, are going to reset their lives with these peptides. That said, the installation of healthy habits has to be there (diet, exercise, etc) or falling back into old, bad, habits will always be a problem. but DAMN does this turn off those negative cravings and allow you to focus on healthy decisions much easier.
English
@grok @kalos21million What about even the article and claims on mechanisms of effects
English
Retatrutide (Reta) is Eli Lilly's investigational triple agonist (GLP-1, GIP, glucagon) for obesity. Phase 2 trial (NEJM 2023): up to 24.2% body weight loss at 48 weeks (12 mg dose) vs ~2% placebo. Early Phase 3 data shows ~71 lbs average loss in select trials.
Facts check out on efficacy from RCTs. Common side effects: GI issues (nausea/diarrhea/vomiting/constipation, mostly mild-moderate, dose-related). Temporary heart rate rise observed. Still not FDA approved; long-term safety data ongoing.
English
I am 39 and very fit / otherwise healthy, was delaying doing them because ApoB was 120 and went to 95 recently. And I was just giving it a few month to experiment with lifestyle and repeat tests. (Before recent times it kept rising despite me doubling down in diet and excrcise.)
Gonna also do heart scan just in case.
And then will start soon. Thank you.
English

If you have very high lipids, I'd do statin/PCSK9 immediately. If you are in the range for weight I'd do GLP1 immediately. There's no reason to wait. Waiting is inconsistent with guideline and evidence, imo.
Guideline says you can elect to wait if you are low background risk and young.
English

Here’s something odd.
Despite the expressed certainty that high LDL is a primary cause driver of atherosclerosis, with claims like “there’s no safe level of high cholesterol” regardless of metabolic state, when I present what seems my own clear-cut case of having a total cholesterol of 700 for nearly 7 years, and then ask a simple question:
How much plaque will be in my arteries?
Almost nobody guesses: “a lot.”
Now, to be clear, this isn’t just a basic coronary artery calcium scan I'm getting. I recently underwent an advanced coronary CT angiography, with expert-guided interpretation and AI-based quantification down to the cubic millimeter (mm3).
Of note, people in their 20s and 30s often do show plaque on these scans, including some well-known nutrition influencers. One example that comes to mind is someone in the plant-based community, in his 30s, with a total plaque volume of 61.3 mm³.
So I come back to the question:
👉How much plaque will be in my heart?
👉And why does it seem that no one wants to guess “a lot”?
These aren’t results I could possibly fake.


English