Sabitlenmiş Tweet

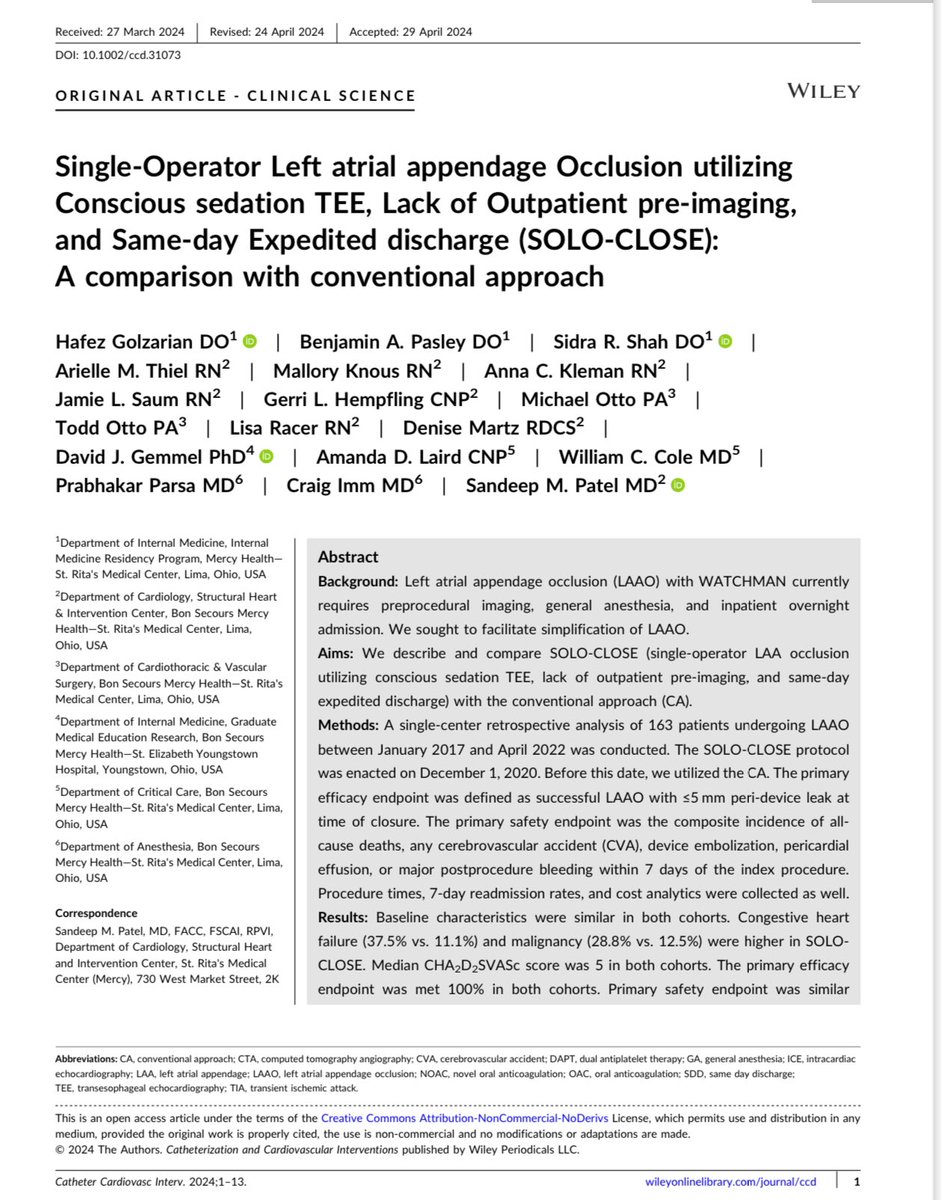
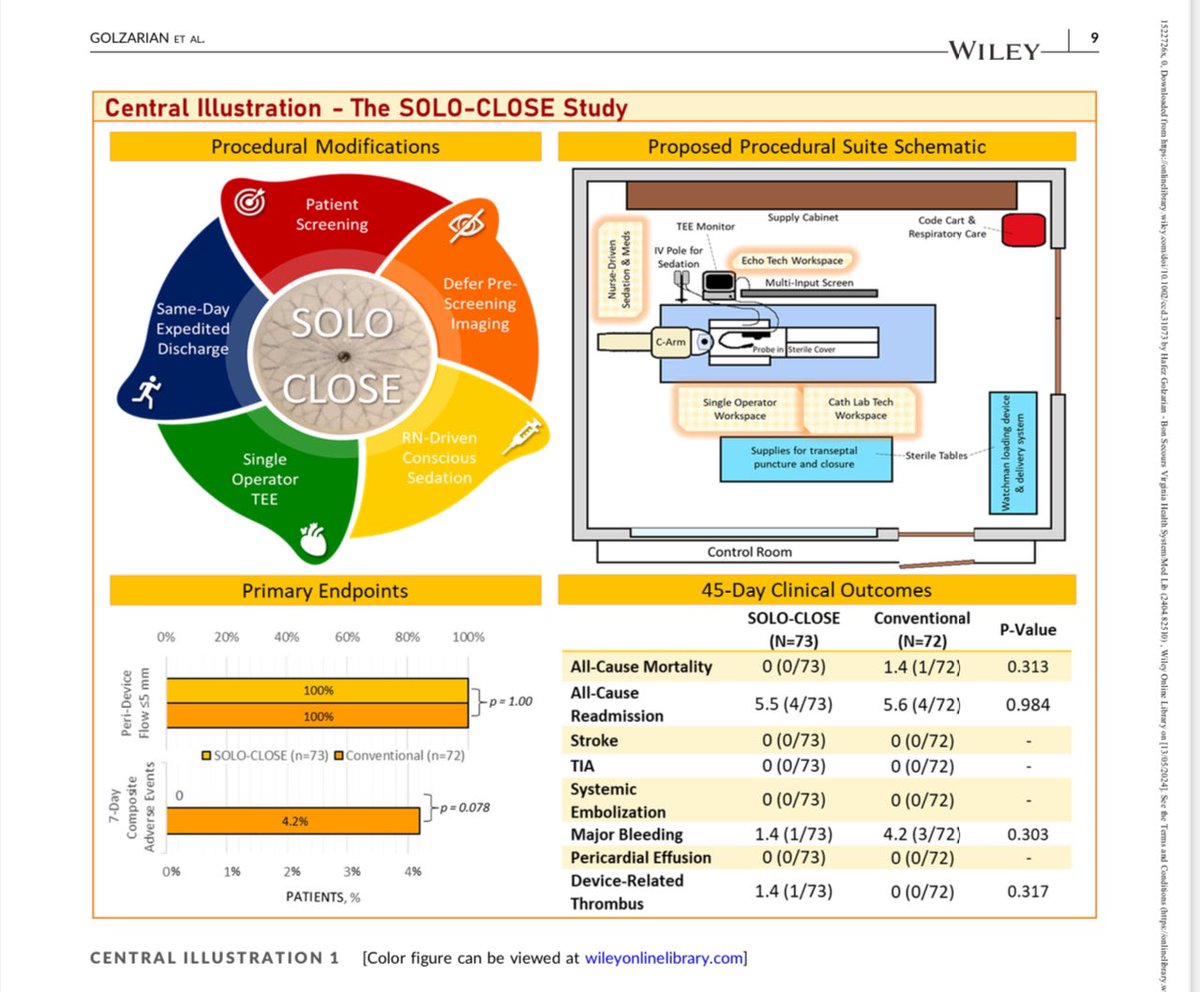
Drumroll please—SOLO CLOSE for WATCHMAN —developed and researched at SRMC—congrats to the team! Live teaching and Virtual Reality cases available from Boston Sci @BSCCardiology @GregMaschi24063 @SCAI @ACCinTouch @TAVRBot @MDT_StructHeart @crfshj @TCTMD
English