Dutch Rojas@DutchRojas
The largest 212 nonprofit hospitals are a danger to the United States of America.
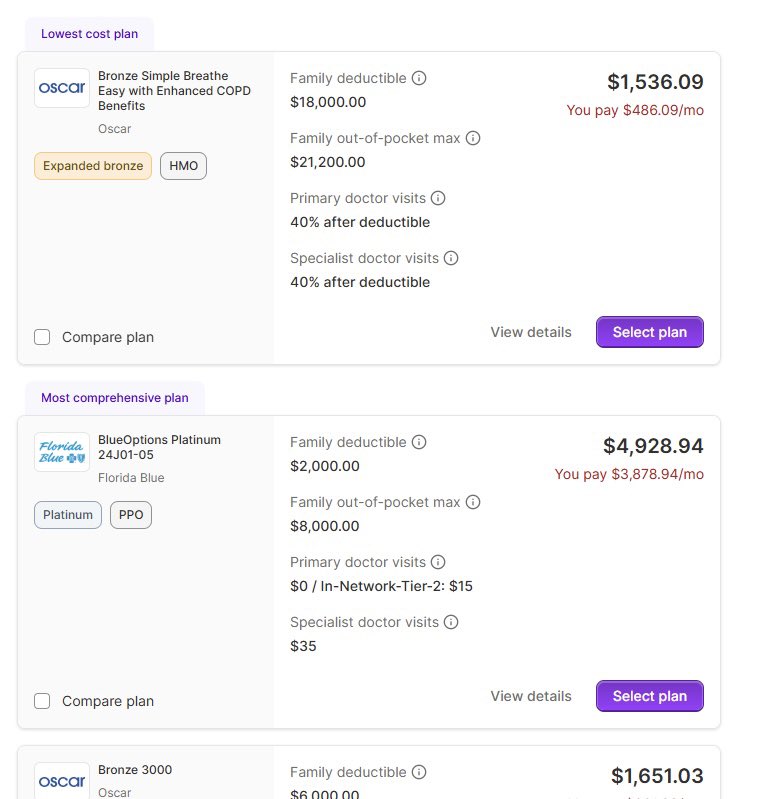
The Centers for Medicare and Medicaid assign them higher reimbursements for the same procedures and treatments performed in a non-hospital setting.
You might say, well they have to take everyone.
I’d agree.
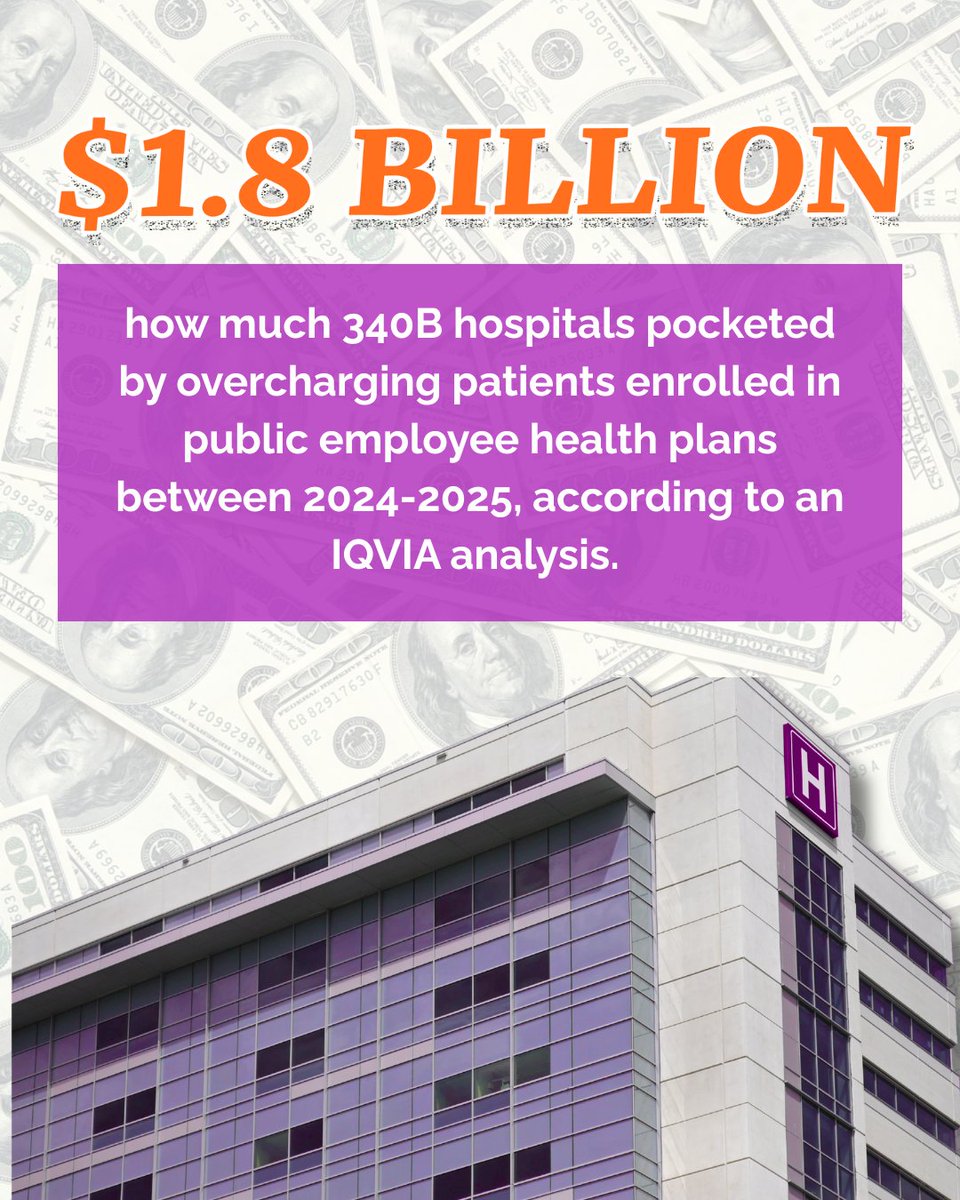
And then I’d teach you a lesson on how they receive 80% of the $275 billion in taxpayer-funded, government-assigned subsidies.
And then I might talk about executive compensation that makes Wall Street blush, jets, trips, and more extravagance, all paid for by taxpayers.
Of these 212 hospital systems, only 2 contribute more in community benefit than they receive in tax benefits.
These same nonprofits pay no property tax, no state income tax, and no federal taxes.
They use those advantages to acquire risk-taking, tax-paying, for-profit businesses and convert them into nonprofits too.
The deal was simple: take care of the community and receive tax abatements.
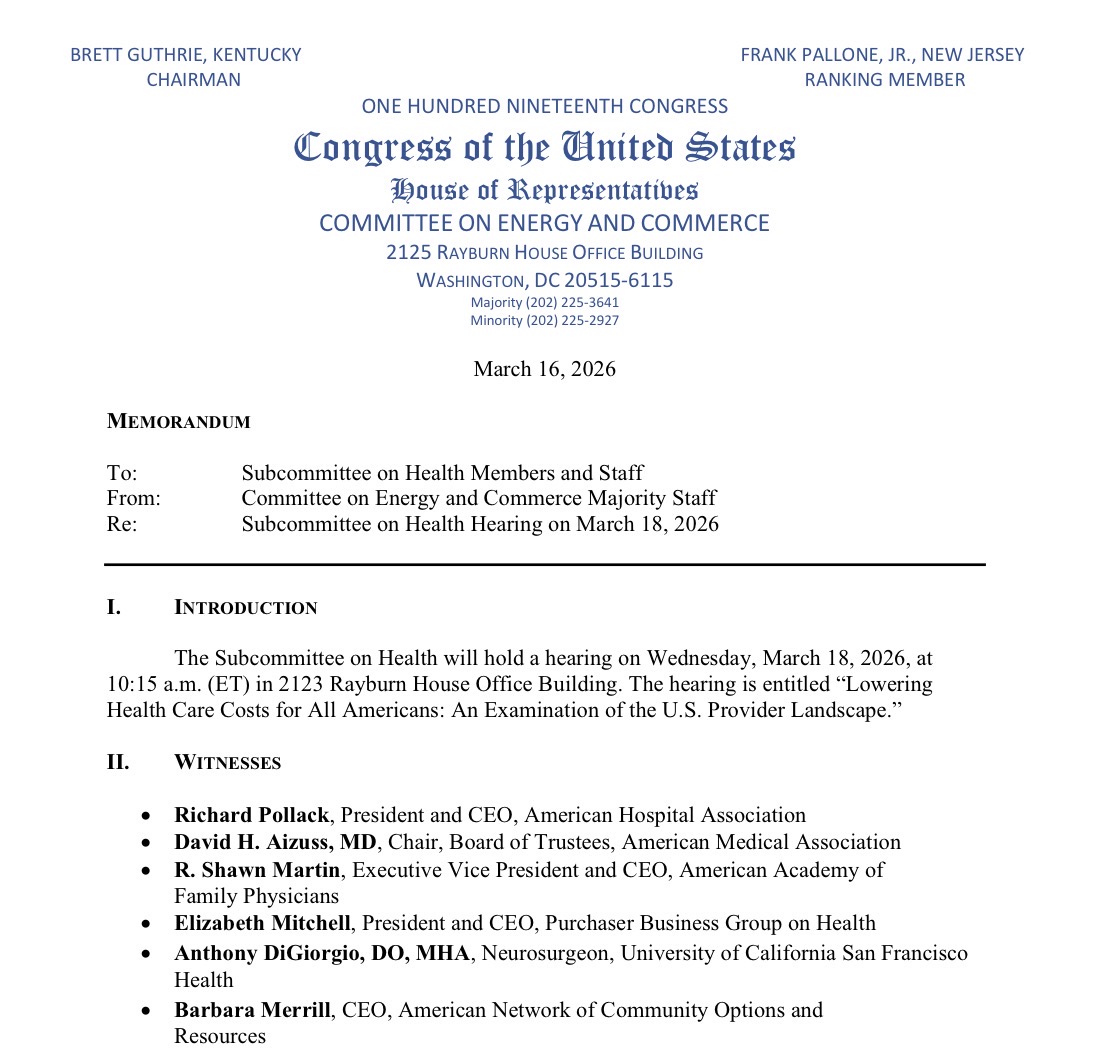
Instead, they broke the deal. And lawmakers, along with a large army of lobbyists, started gaslighting the public.
The nonprofits use the higher reimbursements not to help their communities, but to acquire more independent practices.
And every time that happens, Medicare pays more for the same.
You won’t hear anything from the 7,000 employees or administrators, so don’t expect it.