Sabitlenmiş Tweet

Radical Cystectomy shouldn't be the only conversation after EV-Pembro.


English
Scott E Delacroix Jr M.D.
2.4K posts

@UroCancer
Medical Director Urologic Oncology/GU Cancers. Mary Bird Perkins Cancer Center. Metairie, Louisiana. Bladder and Prostate Cancer subspecialty.

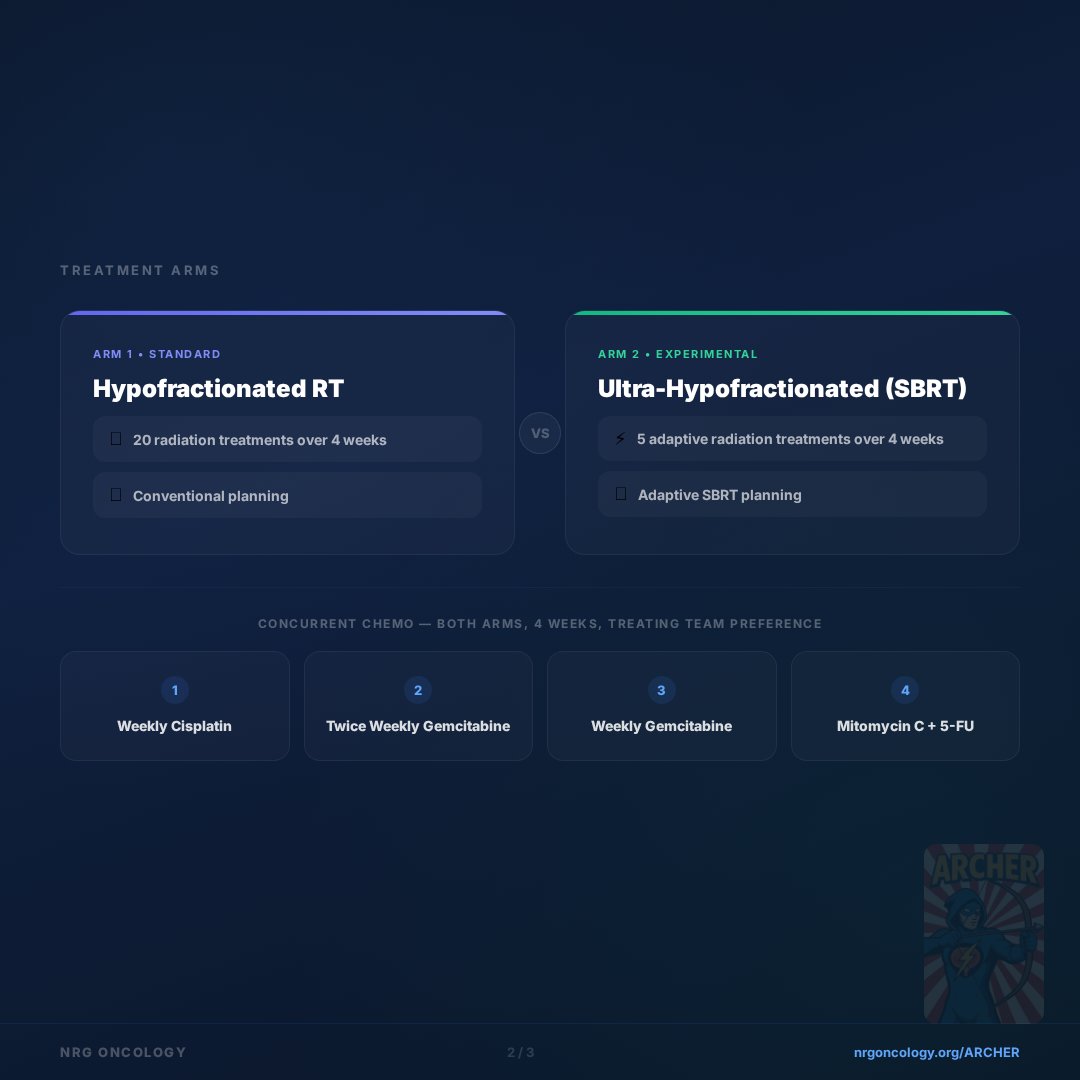
In concert w @BladderCancerUS Think Tank 2026, @NRGonc Podcast on saving the bladder in GU015 (Archer) w @MSKCancerCenter @HimanshuNagarMD & @MBPExcellence @UroCancer! @lauren_henke @DrSpratticus @DrPaulNguyen @wandering_gu @DrRanaMcKay @drjefstathiou @NehaVapiwala





There is still time to register! Go to the member portal for more information. mrlconsortium.org