Sabitlenmiş Tweet

𝗪𝗶𝗻𝘀𝘁𝗼𝗻 𝗣𝗼𝗻
25.2K posts

@WinstonPon
Campaigns • Creative Strategy • Cultural Impact — Founder of Churchill Strategy




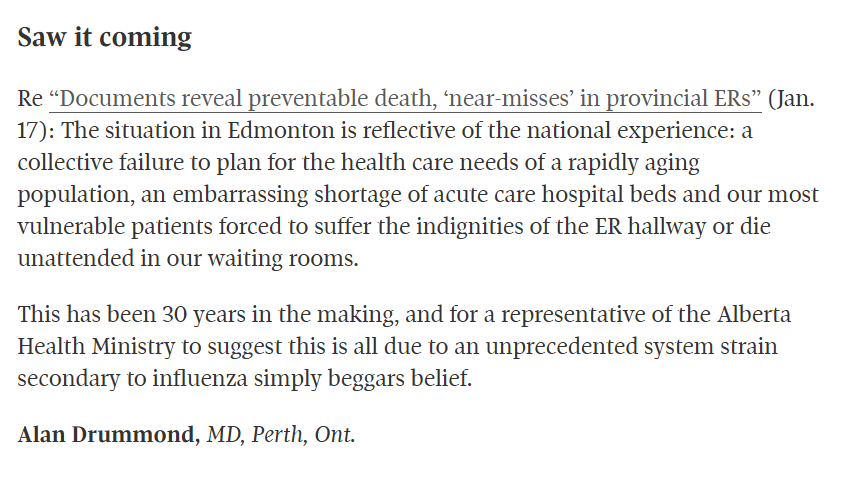
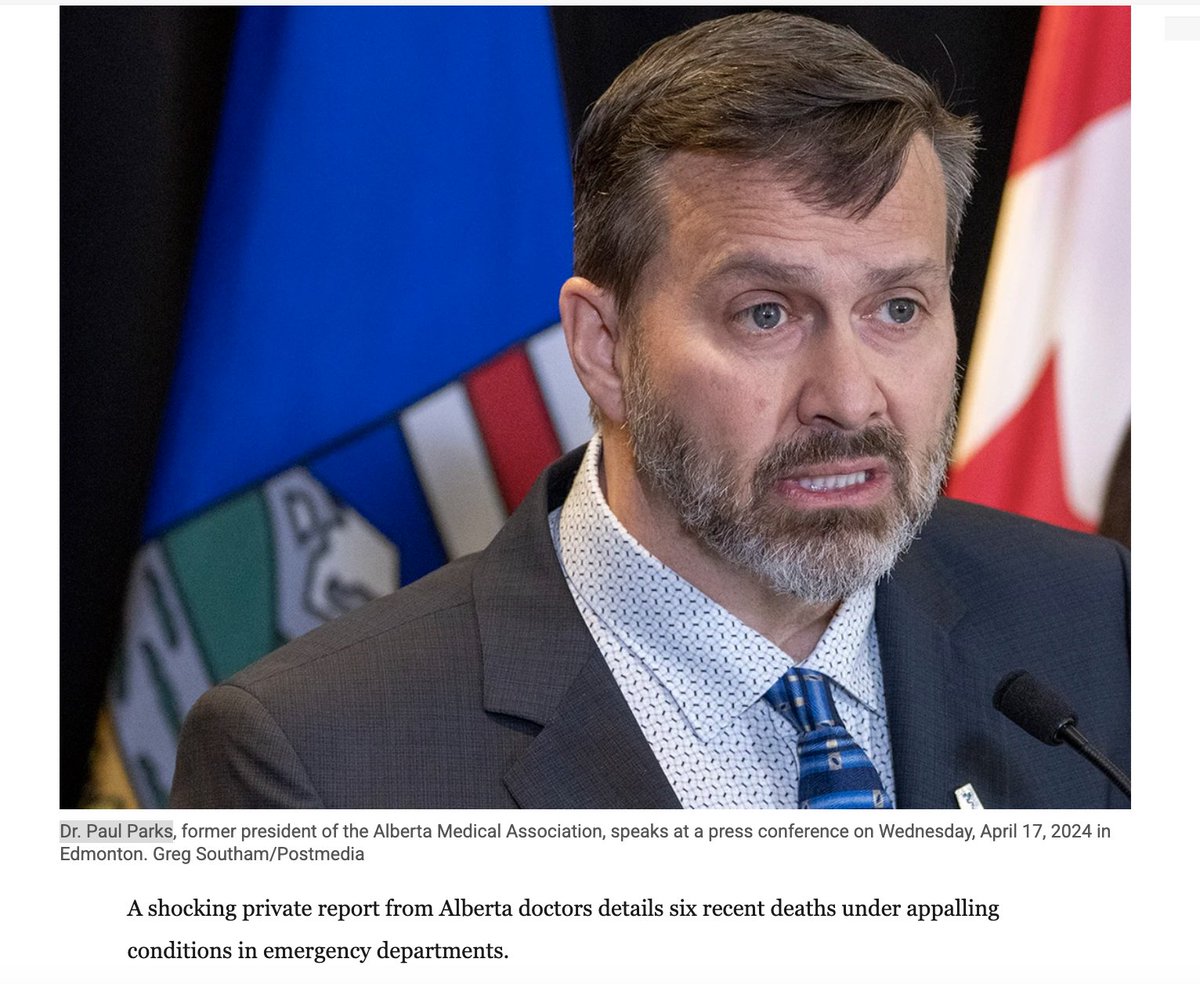
From the DM’s… The Breakdown has obtained a document assembled by ER physicians and sent to the UCP to get them to address the healthcare crisis. We have confirmed its authenticity & that the cases listed have all occurred in the last few weeks. /1 #abpoli #ableg #cdnpoli


LATEST. INTERVIEW. Danielle Smith's hospitals boss fires back, insists health care has not collapsed calgaryherald.com/opinion/column… via @calgaryherald #ableg #abpoli #yyc #cdnpoli #Alberta #abhealth


Ok wait…: 1 - NO! not every admitted pt becomes an ALC. if you can go home post acute care you are DISCHARGED. You go home! that’s the NORM 2 - you ONLY become ALC if you are ready to be discharged but CAN’T go home because you require services not immed, available as an out pt

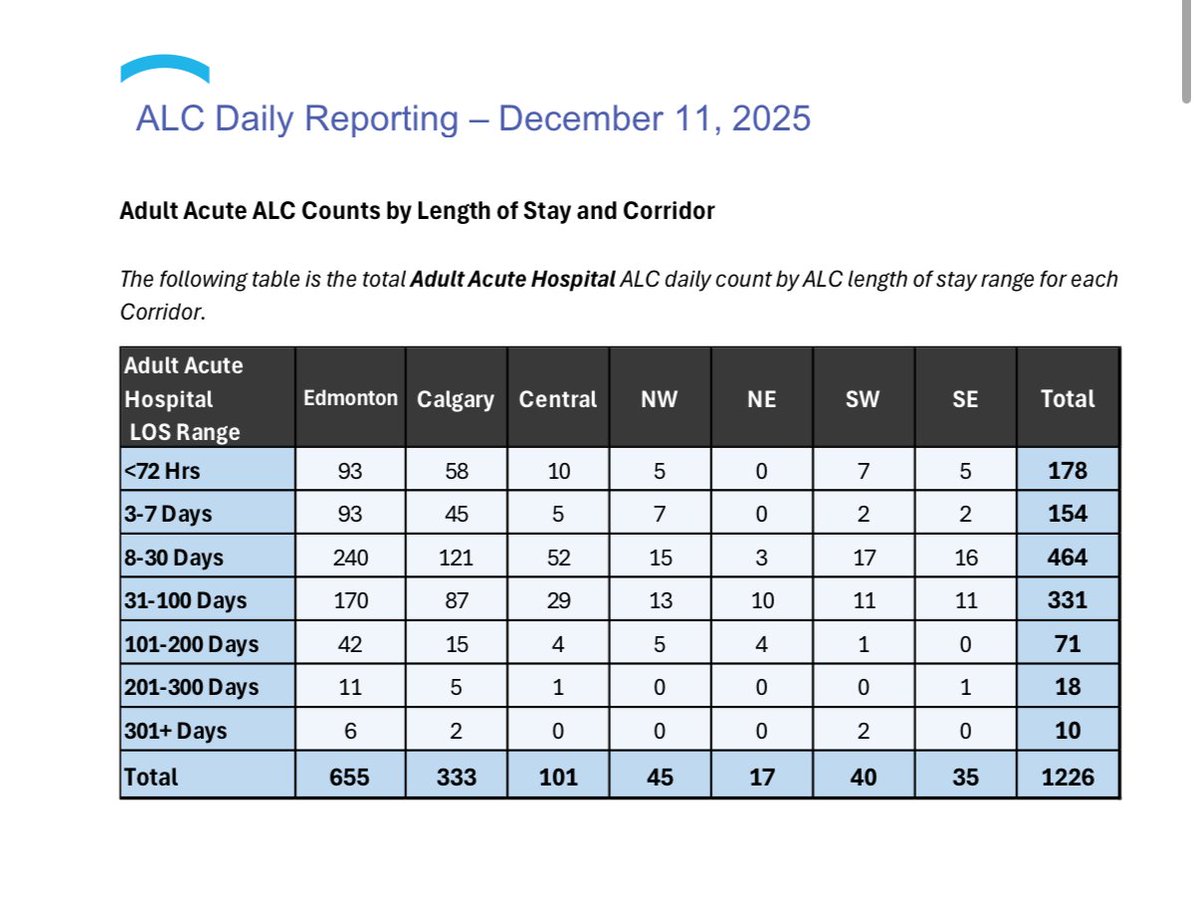



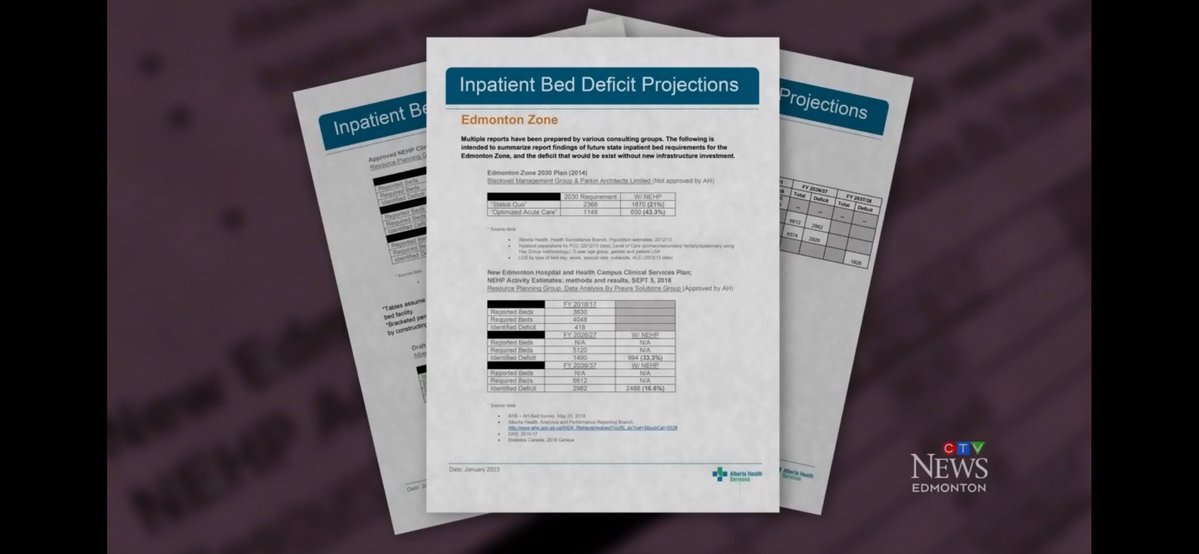
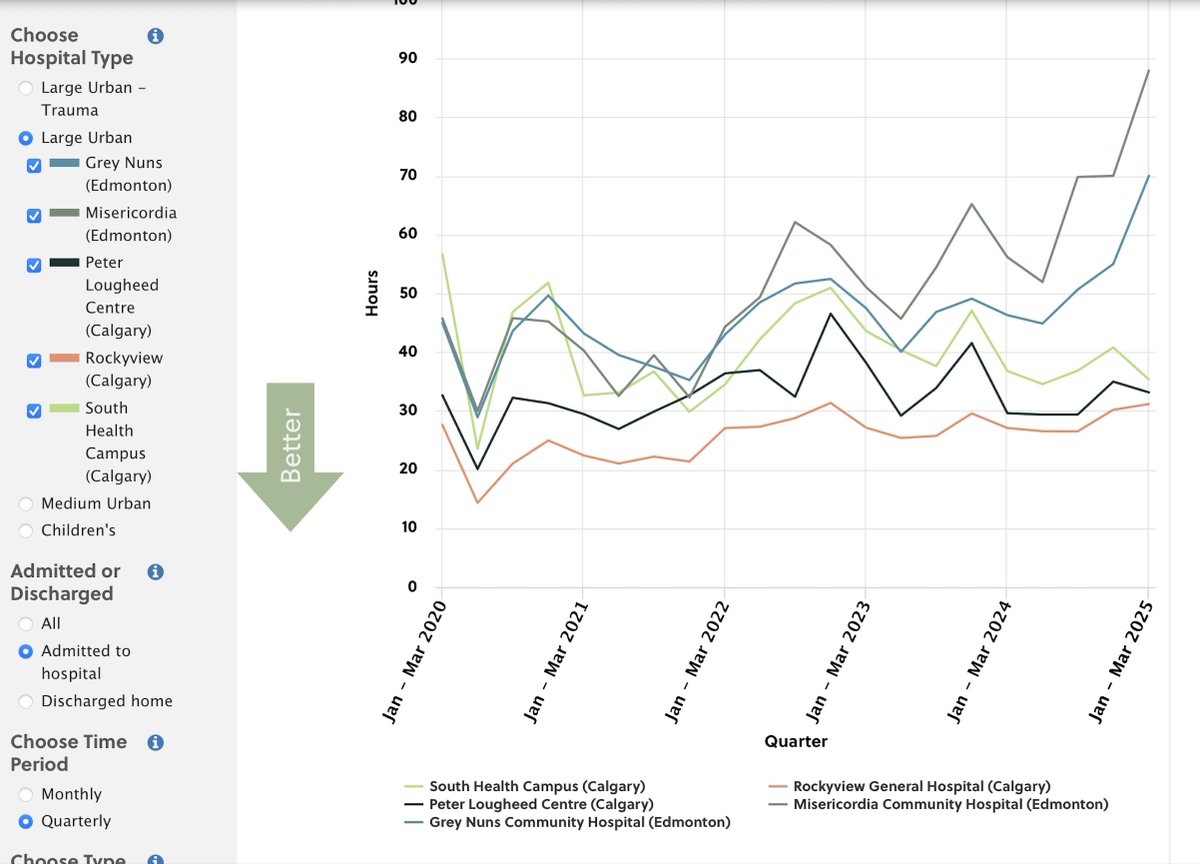
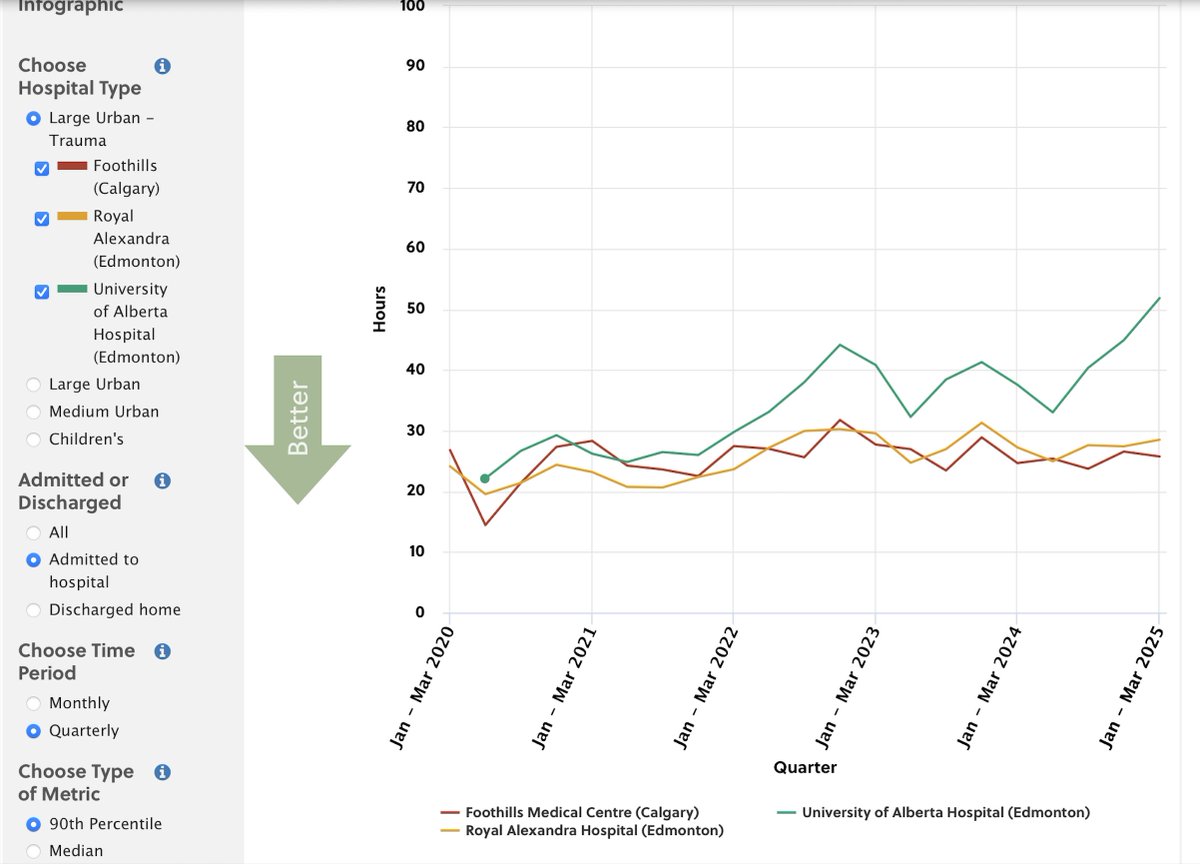
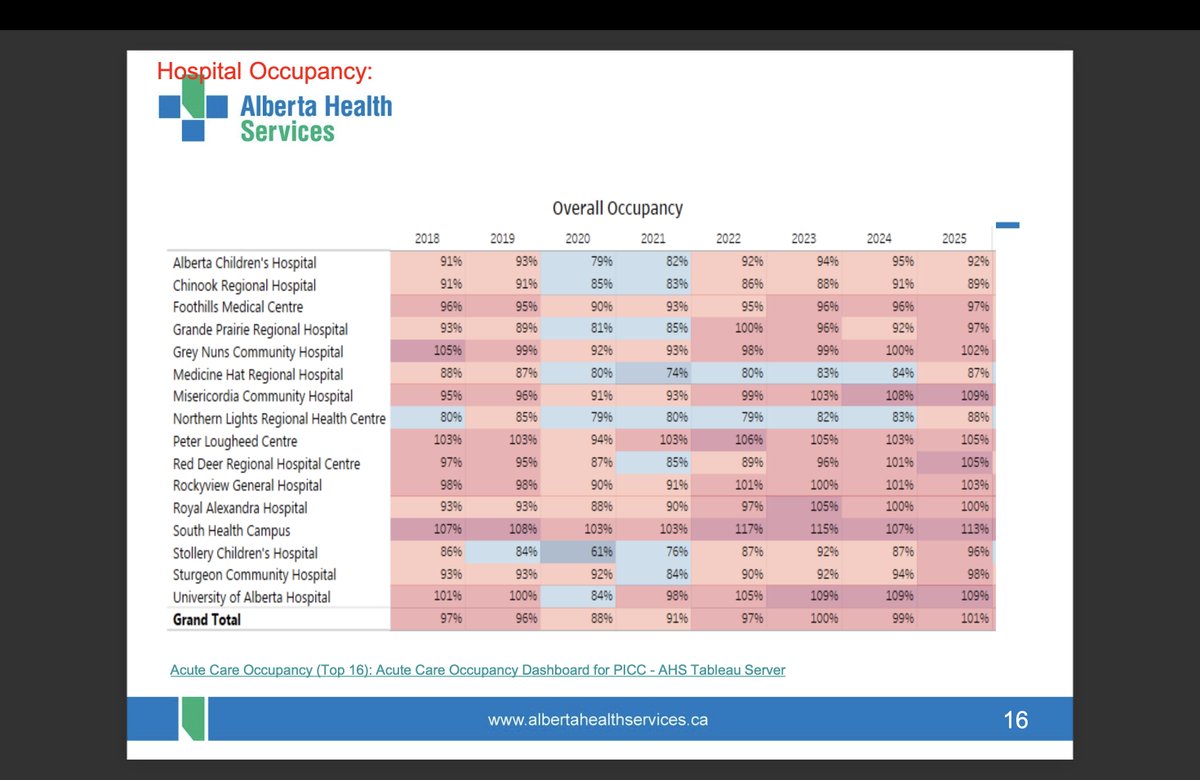
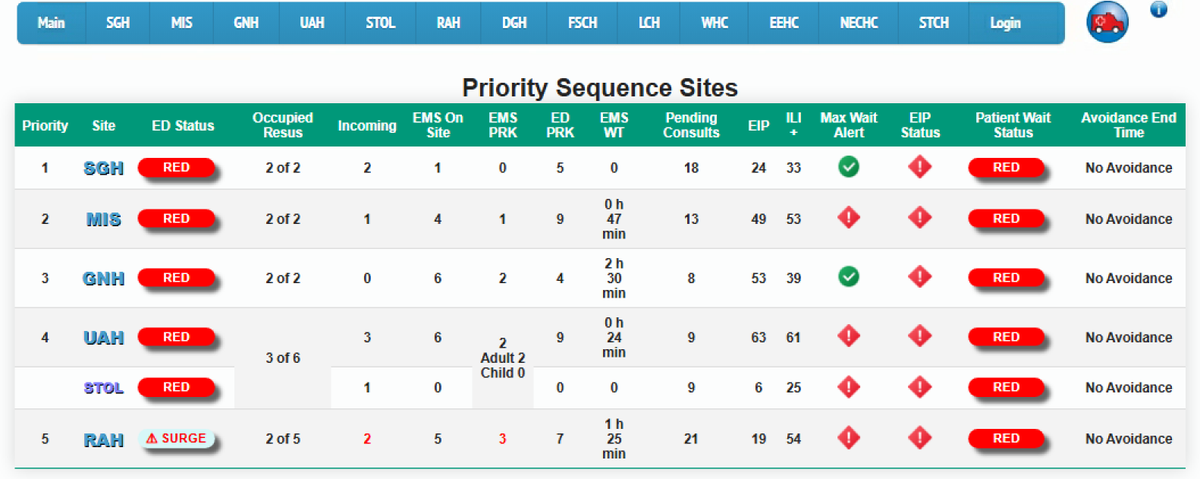
PLEASE REPOST this important reply to Jason Nixon: Minister @JasonNixonAB, I listened to part of your press conference and I commend your efforts to move long-stay ALC patients out of hospital. Thank you. But there are factual inaccuracies that matter. These numbers were given to me by the Premier @ABDanielleSmith on Dec 11 and from AHS August 2025 data. DATA & FACTS: 1. Alberta has ~8,800 acute care beds. 2. Edmonton has ~2,486 adult acute medical beds (not counting pediatrics). 3. Your Dec 11 data shows ~655 ALC patients in Edmonton. Can we agree on that? 4. 655 ÷ 2,486 = 26.3% of Edmonton’s acute beds are occupied by ALC patients. (For context: Grey Nuns + Misericordia together have ~700 adult medical beds.) 5. Edmonton has ~275 ER beds and, two weeks ago, ~255 admitted patients were boarding in those beds, sometimes for days. 6. #YEG receives ~4× the out-of-town transfers compared to #YYC, as it serves a massively underserved Rural North. 7. ERs and major trauma centres are now running out of even a handful of stretchers and hallway chairs. 8. ER bed counts: UofA ≈65, RAH ≈65, Grey Nuns ≈55, Misericordia ≈55. 9. Site-specific ALC numbers: • Aug/25: UofA 158, RAH 192, GNH 69, MIS 120 • Dec 11/25: UofA 163, RAH 118, GNH 80, MIS 75 10. Cause and effect: please explain to Albertans how ALC occupying over one-quarter of acute beds is not driving ER/EMS access block, surgical delays, prolonged waits for critically ill patients, and preventable harm and deaths in waiting rooms. 11. You state ALC is down 15–20%. I’ve confirmed patients were moved, and that is good. 12. BUT many were also reclassified as “acute.” Reclassification does not change ER flow; it moves the goalposts. 13. Ask any paramedic, ER nurse, or ER doctor about “Eviction by 911”: assisted-living and home-care facilities call EMS, patients arrive labelled “failure to thrive,” and providers will not take them back. 14. They then become ALC admissions through the ER, where they rapidly decondition and acquire acute illness. For frail seniors, hospital is often the most dangerous place. Solutions and Advice to Minister (Free of charge): A1. Create a 24/7 multidisciplinary community team linked to ERs to prevent admission of “failure-to-thrive” patients. Care cannot run banker’s hours. A2. When a patient is declared ALC, they must be immediately moved to transitional, rehab, or enhanced home-care pathways (e.g., CHOICE, respite, hospital-at-home). A3. Change the funding model so RNs are on duty 24/7 in assisted-living facilities, connect NPs within PCNs to those facilities, and bring mobile lab and X-ray services to provide higher-level care: like the auxiliary hospitals of the past. Delay converts temporary need into permanent placement. Denmark does this extremely well. Minister, this is not personal and not political. It is math, flow, and patient safety. But incomplete policies are putting the entire acute-care system: rural and urban Alberta at risk. I am unsure why Minister @MattJonesYYC took full responsibility when much of this lies within your portfolio. I welcome an in-person debate on the numbers and the solutions: ANYTIME...ANYPLACE. Healthcare workers: agree or disagree, and please add other solutions. These are only a few low-hanging, low-cost fixes to begin repairing the system. Please pass this on...to encourage respectful debate. @pfparks @JMeddings @BradenMannsYYC @NightShiftMD @raghu_venugopal @TheSGEM @nenshi @TheBreakdownAB @ryanjespersen @cspotweet @DonBraid @RickBellwrites @Alberta_UCP @albertaNDP #AbHealthCrisis #StateofEmergency #ALC #PatientSafety