Zen⚡️Chu ⛑🏴☠️🇺🇸 retweetledi

OpenEvidence started as the place clinicians go to find clinical evidence. Now they're becoming the place medical societies go to CREATE it - that's a whole new moat for winning the AI CDS market. My 5 thoughts...
First, the gist of what OpenEvidence announced:
→ The American Academy of Otolaryngology-Head and Neck Surgery Foundation (AAO-HNSF) and OpenEvidence have partnered to keep clinical practice guidelines current using AI-augmented literature surveillance
→ OpenEvidence built a custom methodology with AAO-HNSF that systematically compares existing guideline recommendations against current medical literature.
→ The system flags specific recommendations for review when new evidence either supports revising the existing guidelines or reaffirms it.
→ AAO-HNSF has already applied this to several of its existing clinical practice guidelines. The goal is to make it easier and faster for societies to keep guidelines up-to-date.
My 5 thoughts on this strategy and what it means for the AI CDS industry:
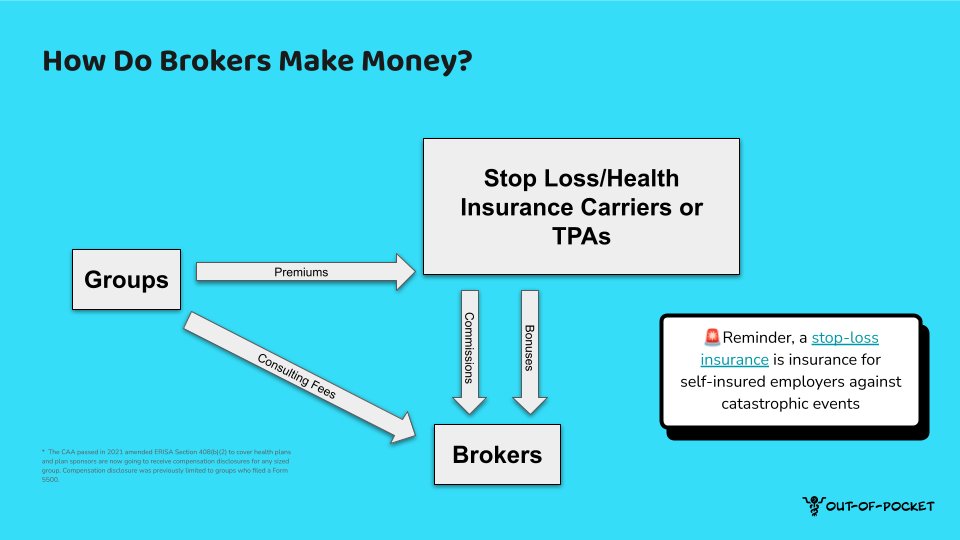
1/ OpenEvidence has strengthened its market position by going beyond simply licensing clinical content from medical societies and journals. By creating a way to add value to medical societies directly, and thus create some dependency for medical societies on OE, it incentivizes those societies to encourage their members to choose OE over other tools.
2/ This is awesome for clinical guideline maintenance. Many clinical practice guidelines become outdated because too many years can go by without a review or updates simply because doing a review is very time and labour intensive. It’s increasingly difficult because the pace of research outpaces our ability to incorporate them into guidelines. By reducing friction to making such updates, we will see guideline updates skyrocket.
3/ In the past, some clinicians may have minimized the value of guidelines because they could be quickly out of date. But if these tools can truly make guidelines more current, the clinician community will be even more willing to use them. This will lead to better patient care.
4/ This puts OE on a potential path to expansion beyond simply evidence search and curation and into opportunities of evidence generation itself. OE is starting by helping to update guidelines, but what if OE creates AI tools to suggest and draft not yet developed, brand new guidelines in the first place? That seems inevitable and the smart thing to do.
5/ This illustrates one of the powerful things about startups. OE has the freedom and courage to try new stuff like this very easily - how do the large incumbents move quickly enough to not just catch up but lead the way on product innovation? Unlike a big entrenched EHR, it’s hard to see how CDS products - even legacy ones - have much of a moat.
English