Sabitlenmiş Tweet
Sean
1.9K posts

Sean
@addingdecades
Life's too short, age better.
Texas or an island far away Katılım Nisan 2025
191 Takip Edilen326 Takipçiler
@Mark_Sisson 💯 also people are still waiting for magic pills when massive action was the solution all along, and likely will never be bypassed
English

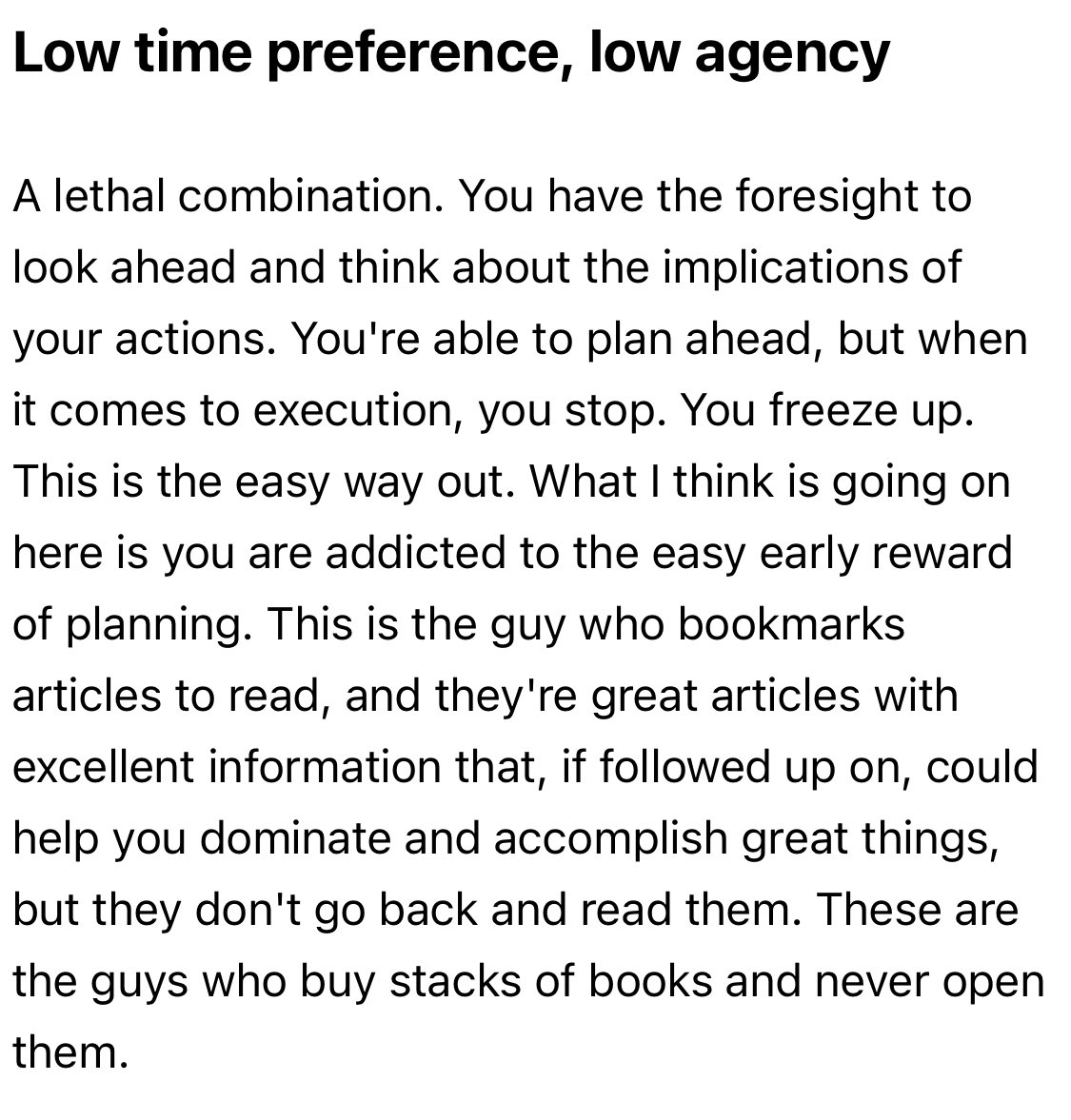
Future Orientation isn’t enough. You must also have the agency and urgency to seize and appreciate the present moment.

Erik@e_cdalton
@Mark_Sisson on the dangers of too much visualization
English
@DanielGilr44222 To be fair, nobody who cares about their health eats from any chain restaurants, fast food or otherwise 🍟 🍔 🤮
English

@dr_edwardgroup Fenbendazol, fortnight. Every reason to gobble it and no reason not to
English

I’ve been talking about parasites since the early 90s. 🪱
Medical literature demonstrates hundreds of cases of parasitic infections mimicking other diseases, especially cancer.
In my opinion, 97% of all c-words are parasitical.
This is why for decades, I’ve encouraged people to look beyond symptoms and ask one question:
What is the root cause?
Too many people spend years chasing diagnoses while never addressing the environment inside the body that allows chronic health issues to take hold.
Whether it’s parasites, toxins, or heavy metals, it all comes down to a toxic internal and external environment.
That’s why I’ve dedicated my life’s work to teaching people how to support the body naturally and create an environment where it can heal from anything.
Here’s a link to my FREE 6 Secrets to Total Body Detox course to help you begin your root-cause healing journey: ghi.ac/6-secrets-to-t…
Blessings and truth,
Dr. Edward Group, DC
#parasitecleanse #parasites #holistichealth #detox #rootcausehealing
English
@ultrarrow There are no legitimate conflicts between nations, today. Every war is a charade between oligarchs and mafias, toward their mutual benefit.
English

🇷🇺 Vladimir Putin:
ABD'de Bay Soros diye bir figür var; küresel ölçekte hemen her şeye karışıyor. Ancak ABD Dışişleri Bakanlığı'na bunun nedenini sorarsanız, bununla hiçbir ilgileri olmadığını ve tüm bunların Bay Soros'un kişisel faaliyetleri olduğunu söylerler.
Türkçe

Bryan Johnson
- Regrets taking an mRNA vaccine
- Acknowledges he was manipulated by health authorities
- Now discovers he has an autoimmune disease where his own immune system is attacking his stomach lining
- Doesn't connect these dots publicly — at least not yet
I can assure you, it is well established that vaccines can cause auto-immune disease.
Vaccine-induced autoimmunity isn't some fringe speculation. The phenomenon has a name in the literature: ASIA syndrome (Autoimmune/Inflammatory Syndrome Induced by Adjuvants), first characterized by Israeli immunologist Yehuda Shoenfeld. The basic mechanism:
Molecular mimicry — vaccine antigens can resemble self-proteins, causing the immune system to attack its own tissues
Adjuvant stimulation — aluminum adjuvants (still used in many vaccines) are designed to provoke strong immune activation, and in susceptible individuals this can break self-tolerance
Bystander activation — the inflammatory cascade can awaken dormant autoreactive T-cells
The stomach's parietal cells express the proton pump H+/K+H^+/K^+H+/K+-ATPaseATPaseATPase, which is the primary autoantigen in AIG. Cross-reactivity between microbial or vaccine antigens and this enzyme is a documented pathway for autoimmune gastritis to develop.
Bryan Johnson@bryan_johnson
Bad news #1: I have an autoimmune disease. My stomach is eating itself. Bad news #2: 2–5% of people have this, too. Likely more, because it hides. Good news: I'm going to try and solve it. Will share all. As a kid, I ate sugar cereal, drank sugary soda, and gobbled down fast food. I had a few healthy years in my early 20s but then became a young father of three and began building a business. Juggling that stress and grind, I let my health slip and gained 40 lbs. Within a few years I’d fallen into a deep, chronic depression. Somewhere in that timeline, my body began developing an autoimmune process affecting my thyroid and then my stomach lining. It’s called Autoimmune Gastritis (AIG). My hypothyroidism got diagnosed when I was 21 years old with a routine blood draw. That enabled me to begin proactive management, supplementing levothyroxine and Armour Thyroid. They are the hormones my body should be producing on its own but wasn’t. By taking these pills daily, my body was able to operate as though my thyroid was functioning properly. What I didn’t know was that something else was going on inside my body: my stomach had begun attacking itself. But there was no routine test to find out and I didn’t have any symptoms. I just discovered it in May. I'm unsure how long I've had it. AIG causes irreversible damage: nutritional deficiency, anemia, and over a long horizon, elevated cancer risk. When AIG is discovered today, standard medical care concedes defeat, stating that nothing can be done except managing the condition, no matter how awful or lethal the effects. Looking back over the past few years, I can now see the early signals we were picking up in measurement but hadn’t connected the dots. For 11 years, I’ve had low ferritin, without anemia. We continually tried to raise my iron levels with food and supplementation but nothing would work. We chased the obvious solutions first. A plant-based diet means all my iron is the hard-to-absorb, non-heme kind. Hard training, sauna, and hyperbaric oxygen all raise the body's demand for iron. But none of them explained the core failure: despite me taking iron orally, trialing every formulation, and using every timing trick, none of the iron would stick. What I didn’t fully appreciate until recently is how many stones my previous providers had left unturned. The low ferritin kept getting explained away but not fixed. I overhauled my medical team earlier this year. It was the rebuild to lay the groundwork for Immortals Care, our $1M a year protocol. With greater capacity, we revisited everything. On the surface, my low ferritin was easy to dismiss by most standards of care. My hemoglobin and hematocrit were normal. Ferritin measures stored iron, while hemoglobin measures circulating iron, and because the body drains its reserves first to keep hemoglobin normal, you can be fully iron deficient with a perfectly normal hemoglobin and hematocrit. This is why my low ferritin kept getting dismissed: the numbers that define anemia looked fine, so no one asked why my iron reserves wouldn't refill. My team pressed on that question. They first turned to a colonoscopy. I was 48 years old and overdue. It was good health hygiene to have while also serving a specific purpose of searching for a hidden source of blood loss such as a polyp or even cancer in my bowels. Either one of those would be an explanation of why the iron kept disappearing. At the same time, they began connecting the dots. Iron absorption depends on stomach acid, so one theory was that my stomach acid was disrupted. They also knew that thyroid and stomach autoimmunity often travel together, so often that the pairing has a name: thyrogastric syndrome. Put against my 27+ year history of autoimmune thyroid disease, the pieces pointed to a single hypothesis: my own immune system was attacking my stomach. To our surprise, my colonoscopy came back clean. A perfectly healthy colon, better than 95% of colonoscopies of men, according to the gastroenterologist. That ruled out the first concern and worst possible outcome: slow continuous bleeding from colon cancer, or pre-cancerous polyp. My team had exercised great foresight though, anticipating this possible outcome. In addition to a colonoscopy, they’d ordered an upper endoscopy to be performed at the same time. The combined procedure is a bi-directional endoscopy. Probes would look at my entire intestinal tract, up from below and down the throat. Additionally, we had several blood biomarkers measured ahead of the procedure to try and pick up on any signals that would give the gastroenterologist guidance for what to look for while doing visual inspections. Fifteen minutes before the procedure, my blood results returned, finding elevated levels of anti-parietal-cells-antibodies (APCA). They came back at roughly five times the upper limit of normal (103, against a ceiling of 20 Units/mL). It was a positive result confirming the suspicion of AIG being the culprit behind my low ferritin, the other type of gastritis, driven by a bacterial infection, was already ruled out, as we knew I am negative to H. pylori. Even before this finding, my team had ordered five biopsies to be taken from three regions of my stomach. The biopsies were the critical piece. Had they not been ordered, the bi-directional endoscopy would have been completed and AIG remained undiagnosed as there were no visual signatures of the condition in my intestines. Two days later, the results of biopsies came in, showing clear signs of early autoimmune gastritis: early atrophy confined to the acid-producing lining, with the rest of the stomach still spared. My team had anticipated this, methodically tracing every line of evidence. We now had a formal diagnosis. I have autoimmune gastritis AIG. My stomach is eating itself. So this was never one problem. It was three, linked to one another: the iron deficiency, the autoimmune gastritis driving it, and the autoimmune thyroid disease alongside it. Iron and thyroid feed each other both ways, low iron impairs the conversion of thyroid hormone into its active form, and an under active thyroid impairs how the body uses iron. Each made the other harder to fix. Autoimmune gastritis affects an estimated 2–5% of people, and likely more, because it hides and is challenging to diagnose. It's usually silent for years, surfacing only once the stomach has atrophied enough to do real damage: iron deficiency first, then B12 deficiency, then anemia from both, and over a long horizon, raised stomach-cancer risk. In one study of people with precancerous gastric lesions, roughly 18% carried the autoimmune antibodies, and only about 1% had ever been diagnosed. And the earliest clue, low ferritin, is the one standard medicine waves through. Low iron stores get normalized and rarely investigated at all when anemia hasn't shown up yet. That blind spot is what hid mine for a decade. The good news: the iron deficiency is now corrected. I received a 1,000 mg Monoferric iron infusion. This was chosen for two reasons after considering multiple formulations. First, it can safely deliver a full dose of iron in a single infusion (1,000 mg), while older options like Venofer require several separate appointments to reach the same total. Second, certain other IV iron formulations can cause a drop in blood phosphate levels, an important mineral for bones and energy. Monoferric is much less likely to do this, which matters given how closely we track long-term metabolic and bone health parameters. As mentioned earlier, current medical standards treat AIG as something to be managed, not resolved. It's worth noting that many of you give me a hard time, inviting me to "live life" and engage in self-destructive behaviors like a "normal person". I'm cool with the playful ribbing. Also, had I not taken care of my health during the past five years, my situation could potentially be very serious. You too may have a lurking health issue that is undiagnosed and could increase in severity from unhealthy life choices, without your knowing. The absence of symptoms is not the presence of health. A gentle nudge that minding your health, no matter your situation in life, is good decision making. My team and I are going to try and solve my AIG. This is how we’re approaching it: First, routine monitoring keeps the disease in view: ferritin and iron, B12, the pepsinogen I/II ratio, gastrin, and chromogranin A. Gastrin is the dial to watch. If it climbs, the disease is advancing, and the risk of gastric neuroendocrine tumors climbs with it. Second, we’re doing advanced characterization of the disease. We’ll do a repeat biopsy to read the immune infiltrate, deep cytokine profiling, and T-cell subset analysis, to see which pathways are actually firing. That testing drives the intervention plan, including the experimental approaches we intend to develop. + If gastrin and chromogranin rise: damp the gastrin drive (netazepide) and tighten endoscopic surveillance. If the profile is Th1 / interferon-driven: target JAK/STAT. + If it's Th17 / IL-17-driven: target IL-17 and STAT3. + If regulatory T cells are failing: rebuild them (low-dose IL-2, induced Tregs). + If it's antibody- and B-cell-driven and antigen-specific: engineered cell therapy (CAAR-T). Which organizes into four tiers, from available today to frontier: Tier 1, now: protect and support; zinc-L-carnosine, and acid replacement (betaine HCl with pepsin) under physician supervision. This is specific to my case and not something to self-prescribe, especially given the cancer-surveillance considerations above. Tier 2, target the signaling , JAK/STAT, GSK-3, IL-17, and damp the gastrin drive (netazepide). Tier 3, reset the cells, induced regulatory T cells (iTregs). Tier 4, frontier: engineered T-cell therapy (CAR-T / CAAR-T), custom AI-designed antibodies, or synthetic proteins, that can specifically seek out inactivate or destroy the rogue immune cells attacking my stomach lining. To be clear: there's no approved cure for autoimmune gastritis today. Medicine treats it as something to manage, not solve. Tiers 2 through 4 are investigational preclinical evidence at best, and in several cases therapies that still have to be built. If you're working on autoimmune gastritis, antigen-specific tolerance, regulatory T cells, or CAAR-T for organ-specific autoimmunity, please reach out. Modern medicine has normalized too many conditions that erode our health, function, and comfort, shrinking the goal to monitoring and management while a cure is rarely even attempted. Most of these verdicts were handed down decades ago, in an era that predates nearly all of our current tech and science, and they have gone largely unchallenged. We want to change that. In the age of AI, multiomics, and custom-built DNA, proteins, and cells, no condition should be presumed incurable simply because no one has yet tried to cure it with today's stack. I’ll end on a personal note. We fill our days mostly on things that are trivial next to what we ultimately care about. We know, deep down, however, that in the noise of it all, health is easily forgotten until it’s the only thing that matters. We spend a fraction of our lives truly sober to the preciousness of life. We feel it when someone we love dies, when a child is born, when we come close to death ourselves, or when a diagnosis marks our limit. In those moments, we are sobered, and the rarity of it all becomes self evident. Imagine the existence we’d build together if that clarity didn’t fade. I wish all of you the very best. Care for yourself, care for others, care for the planet and care for our animal friends. Care for life as it’s the most precious gift there is.
English
@DavidBCollum Ah, that's reassuring
Wake me up from cryo-stasis, after population declines 90%.
Nothing stops Global Mouse Utopia.
Health, Wealth, Family. Stay focused.
English
Email exchange...
Me: The bottom line is that the entire system is hopelessly corrupt.
Response: I don’t think it’s the entire system. It’s just the Congress, the CIA, the FBI, the FDA, the CDC, the military industrial complex, big pharm, big climate, both parties, AIPAC, the public unions, silicon valley, and possibly a few other things.
English
@Mangan150 Well, this level of blindness is appropriate for very religious people. Who is surprised
#1 Trendy diet to feed narcissistic supply
#2 pretend to be results oriented
English
Bryan Johnson looks at massive numbers of biomarkers regularly, takes all kinds of supplements, and pays great attention to what he eats.
And if he can't make veganism work, what hope is there for others making it work?
English
@bryan_johnson People love suffering and failure, and attention.
Could just have some bone broth and tiptoe back into an animal based diet. But this plant-based struggle is more fun apparently, because it justifies analysis posting? 🤔
English

Massive blood draw today:
> decoding 1 million immune cells
> identifying the rogue clones attacking my stomach
> causing the autoimmune gastritis
This is incredible technology.
Think of your immune cells as trillions of soldiers. Each carries a unique key designed to unlock and destroy a specific threat, like a virus or bacteria.
A standard blood test allows you to see how many soldiers you have, but not their keys. Sequencing 1 million individual immune cells allows us to read the exact pattern of the teeth on every single key.
This is important for my autoimmune gastritis (AIG) because a specific platoon of rogue soldiers has developed keys that unlock an attack on my stomach lining.
Right now, we don’t know who they are. This test will inform us of which soldiers have gone rogue and are attacking me from within.
Once we know soldier and key, we know what therapy path to pursue to shut them down.
Other makers in this blood draw:
Ferritin, Soluble Transferrin Receptor, Iron and TIBC, Transferrin Saturation, Erythropoietin (EPO), Reticulocyte Count, CBC With Differential/Platelet, Phosphorus, Comprehensive Metabolic Panel (14), Antiparietal Cell Antibody, Intrinsic Factor Abs, Gastrin, Chromogranin A, Celiac Ab tTG IgA w/Rflx, IL-2 Receptor Alpha, T- and B-Lymphocyte/Nat Killer, Complement C3, Complement C4, Tumor Necrosis Factor-Alpha, Interleukin-6, HLA DRB1/3/4/5/DQB1, Cardiometabolic Report, Total Glutathione, Selenium, Coenzyme Q10, Oxidized LDL, Essential Fatty Acid Profile, Lp-PLA2 Activity, Myeloperoxidase (MPO), Vitamin D 25-Hydroxy, Magnesium, Copper, Zinc, Vitamin B12, Methylmalonic Acid, Folate, Hemoglobin A1c, GlycA, Fructosamine, C-Reactive Protein Cardiac, NT-proBNP, Lipid Panel, Apolipoprotein A-1, Apolipoprotein B, NMR LipoProfile, Lipoprotein (a), p-tau217, S-100B Protein, Neurofilament Light Chain, Glial Fibrillary Acid Protein

English
@FoFtyTrader I recall a documentary about 20 years ago where two newbie brokers in Manhattan were hocking SanDisk, saying this is make or break for their careers....oops
English

UPDATE: i fired my broker.
he lied, there was no special bonus after the RSI hit 100

FoFty@FoFtyTrader
my broker called again - he promised me this time is truly the very best of times to go long sandisk now that its monthly rsi hit 99.2 he said nothing has every gotten this close to 100 in history and that there is a huge bonus payout to bagholders if it ever reaches 100
English
ya I see that's reasonable.
A small amount of UV exposure is probably a net benefit, i.e. Hormesis. If only due to exercising the UVB--> D3 machinery, Nitric Oxide, and stimulated repair of damage.
But that small amount of UV could be less than one second of direct sunlight per week.
English

@addingdecades @Mark_Sisson Mark was saying that protecting his face from UV means his face won't age, but keeping his body open to the rays will help him with Vitamin D. Mark was NOT saying that, generally speaking, UV won't age the face.
English
Bryan should eat oysters and mussels. No nervous systems, no subjective pain being caused, but you get bioavailable DHA, iron, zinc, and copper.
Bryan should start getting more full body sunlight while protecting his face. Face doesn't age from UV, but body creates vitamin D.
Bryan Johnson@bryan_johnson
Bad news #1: I have an autoimmune disease. My stomach is eating itself. Bad news #2: 2–5% of people have this, too. Likely more, because it hides. Good news: I'm going to try and solve it. Will share all. As a kid, I ate sugar cereal, drank sugary soda, and gobbled down fast food. I had a few healthy years in my early 20s but then became a young father of three and began building a business. Juggling that stress and grind, I let my health slip and gained 40 lbs. Within a few years I’d fallen into a deep, chronic depression. Somewhere in that timeline, my body began developing an autoimmune process affecting my thyroid and then my stomach lining. It’s called Autoimmune Gastritis (AIG). My hypothyroidism got diagnosed when I was 21 years old with a routine blood draw. That enabled me to begin proactive management, supplementing levothyroxine and Armour Thyroid. They are the hormones my body should be producing on its own but wasn’t. By taking these pills daily, my body was able to operate as though my thyroid was functioning properly. What I didn’t know was that something else was going on inside my body: my stomach had begun attacking itself. But there was no routine test to find out and I didn’t have any symptoms. I just discovered it in May. I'm unsure how long I've had it. AIG causes irreversible damage: nutritional deficiency, anemia, and over a long horizon, elevated cancer risk. When AIG is discovered today, standard medical care concedes defeat, stating that nothing can be done except managing the condition, no matter how awful or lethal the effects. Looking back over the past few years, I can now see the early signals we were picking up in measurement but hadn’t connected the dots. For 11 years, I’ve had low ferritin, without anemia. We continually tried to raise my iron levels with food and supplementation but nothing would work. We chased the obvious solutions first. A plant-based diet means all my iron is the hard-to-absorb, non-heme kind. Hard training, sauna, and hyperbaric oxygen all raise the body's demand for iron. But none of them explained the core failure: despite me taking iron orally, trialing every formulation, and using every timing trick, none of the iron would stick. What I didn’t fully appreciate until recently is how many stones my previous providers had left unturned. The low ferritin kept getting explained away but not fixed. I overhauled my medical team earlier this year. It was the rebuild to lay the groundwork for Immortals Care, our $1M a year protocol. With greater capacity, we revisited everything. On the surface, my low ferritin was easy to dismiss by most standards of care. My hemoglobin and hematocrit were normal. Ferritin measures stored iron, while hemoglobin measures circulating iron, and because the body drains its reserves first to keep hemoglobin normal, you can be fully iron deficient with a perfectly normal hemoglobin and hematocrit. This is why my low ferritin kept getting dismissed: the numbers that define anemia looked fine, so no one asked why my iron reserves wouldn't refill. My team pressed on that question. They first turned to a colonoscopy. I was 48 years old and overdue. It was good health hygiene to have while also serving a specific purpose of searching for a hidden source of blood loss such as a polyp or even cancer in my bowels. Either one of those would be an explanation of why the iron kept disappearing. At the same time, they began connecting the dots. Iron absorption depends on stomach acid, so one theory was that my stomach acid was disrupted. They also knew that thyroid and stomach autoimmunity often travel together, so often that the pairing has a name: thyrogastric syndrome. Put against my 27+ year history of autoimmune thyroid disease, the pieces pointed to a single hypothesis: my own immune system was attacking my stomach. To our surprise, my colonoscopy came back clean. A perfectly healthy colon, better than 95% of colonoscopies of men, according to the gastroenterologist. That ruled out the first concern and worst possible outcome: slow continuous bleeding from colon cancer, or pre-cancerous polyp. My team had exercised great foresight though, anticipating this possible outcome. In addition to a colonoscopy, they’d ordered an upper endoscopy to be performed at the same time. The combined procedure is a bi-directional endoscopy. Probes would look at my entire intestinal tract, up from below and down the throat. Additionally, we had several blood biomarkers measured ahead of the procedure to try and pick up on any signals that would give the gastroenterologist guidance for what to look for while doing visual inspections. Fifteen minutes before the procedure, my blood results returned, finding elevated levels of anti-parietal-cells-antibodies (APCA). They came back at roughly five times the upper limit of normal (103, against a ceiling of 20 Units/mL). It was a positive result confirming the suspicion of AIG being the culprit behind my low ferritin, the other type of gastritis, driven by a bacterial infection, was already ruled out, as we knew I am negative to H. pylori. Even before this finding, my team had ordered five biopsies to be taken from three regions of my stomach. The biopsies were the critical piece. Had they not been ordered, the bi-directional endoscopy would have been completed and AIG remained undiagnosed as there were no visual signatures of the condition in my intestines. Two days later, the results of biopsies came in, showing clear signs of early autoimmune gastritis: early atrophy confined to the acid-producing lining, with the rest of the stomach still spared. My team had anticipated this, methodically tracing every line of evidence. We now had a formal diagnosis. I have autoimmune gastritis AIG. My stomach is eating itself. So this was never one problem. It was three, linked to one another: the iron deficiency, the autoimmune gastritis driving it, and the autoimmune thyroid disease alongside it. Iron and thyroid feed each other both ways, low iron impairs the conversion of thyroid hormone into its active form, and an under active thyroid impairs how the body uses iron. Each made the other harder to fix. Autoimmune gastritis affects an estimated 2–5% of people, and likely more, because it hides and is challenging to diagnose. It's usually silent for years, surfacing only once the stomach has atrophied enough to do real damage: iron deficiency first, then B12 deficiency, then anemia from both, and over a long horizon, raised stomach-cancer risk. In one study of people with precancerous gastric lesions, roughly 18% carried the autoimmune antibodies, and only about 1% had ever been diagnosed. And the earliest clue, low ferritin, is the one standard medicine waves through. Low iron stores get normalized and rarely investigated at all when anemia hasn't shown up yet. That blind spot is what hid mine for a decade. The good news: the iron deficiency is now corrected. I received a 1,000 mg Monoferric iron infusion. This was chosen for two reasons after considering multiple formulations. First, it can safely deliver a full dose of iron in a single infusion (1,000 mg), while older options like Venofer require several separate appointments to reach the same total. Second, certain other IV iron formulations can cause a drop in blood phosphate levels, an important mineral for bones and energy. Monoferric is much less likely to do this, which matters given how closely we track long-term metabolic and bone health parameters. As mentioned earlier, current medical standards treat AIG as something to be managed, not resolved. It's worth noting that many of you give me a hard time, inviting me to "live life" and engage in self-destructive behaviors like a "normal person". I'm cool with the playful ribbing. Also, had I not taken care of my health during the past five years, my situation could potentially be very serious. You too may have a lurking health issue that is undiagnosed and could increase in severity from unhealthy life choices, without your knowing. The absence of symptoms is not the presence of health. A gentle nudge that minding your health, no matter your situation in life, is good decision making. My team and I are going to try and solve my AIG. This is how we’re approaching it: First, routine monitoring keeps the disease in view: ferritin and iron, B12, the pepsinogen I/II ratio, gastrin, and chromogranin A. Gastrin is the dial to watch. If it climbs, the disease is advancing, and the risk of gastric neuroendocrine tumors climbs with it. Second, we’re doing advanced characterization of the disease. We’ll do a repeat biopsy to read the immune infiltrate, deep cytokine profiling, and T-cell subset analysis, to see which pathways are actually firing. That testing drives the intervention plan, including the experimental approaches we intend to develop. + If gastrin and chromogranin rise: damp the gastrin drive (netazepide) and tighten endoscopic surveillance. If the profile is Th1 / interferon-driven: target JAK/STAT. + If it's Th17 / IL-17-driven: target IL-17 and STAT3. + If regulatory T cells are failing: rebuild them (low-dose IL-2, induced Tregs). + If it's antibody- and B-cell-driven and antigen-specific: engineered cell therapy (CAAR-T). Which organizes into four tiers, from available today to frontier: Tier 1, now: protect and support; zinc-L-carnosine, and acid replacement (betaine HCl with pepsin) under physician supervision. This is specific to my case and not something to self-prescribe, especially given the cancer-surveillance considerations above. Tier 2, target the signaling , JAK/STAT, GSK-3, IL-17, and damp the gastrin drive (netazepide). Tier 3, reset the cells, induced regulatory T cells (iTregs). Tier 4, frontier: engineered T-cell therapy (CAR-T / CAAR-T), custom AI-designed antibodies, or synthetic proteins, that can specifically seek out inactivate or destroy the rogue immune cells attacking my stomach lining. To be clear: there's no approved cure for autoimmune gastritis today. Medicine treats it as something to manage, not solve. Tiers 2 through 4 are investigational preclinical evidence at best, and in several cases therapies that still have to be built. If you're working on autoimmune gastritis, antigen-specific tolerance, regulatory T cells, or CAAR-T for organ-specific autoimmunity, please reach out. Modern medicine has normalized too many conditions that erode our health, function, and comfort, shrinking the goal to monitoring and management while a cure is rarely even attempted. Most of these verdicts were handed down decades ago, in an era that predates nearly all of our current tech and science, and they have gone largely unchallenged. We want to change that. In the age of AI, multiomics, and custom-built DNA, proteins, and cells, no condition should be presumed incurable simply because no one has yet tried to cure it with today's stack. I’ll end on a personal note. We fill our days mostly on things that are trivial next to what we ultimately care about. We know, deep down, however, that in the noise of it all, health is easily forgotten until it’s the only thing that matters. We spend a fraction of our lives truly sober to the preciousness of life. We feel it when someone we love dies, when a child is born, when we come close to death ourselves, or when a diagnosis marks our limit. In those moments, we are sobered, and the rarity of it all becomes self evident. Imagine the existence we’d build together if that clarity didn’t fade. I wish all of you the very best. Care for yourself, care for others, care for the planet and care for our animal friends. Care for life as it’s the most precious gift there is.
English
@Mark_Sisson I mean it's just self-evident that UV accelerates skin aging.
...with all due respect.
But yes skin ages and sags, even with zero UV, but the mechanisms are distinct.
We don't even need to trust dermatologist about the technical details.
English
@zoeharcombe @bryan_johnson He's obviously a very religious man. Dogma first, and pretend to be results focused after that
If you're results fosused any nothing above that, then you'll likely agree that avoiding UV is nearly the only thing Bryan gets right.
English

For someone trying to live as long as possible, @bryan_johnson does plenty of harmful things...
- Covid gene therapies (in other posts)
- Plant-based diet (doesn't provide the essential nutrients in the form he needs them)
- No mention of vit C for iron absorption
- Colonoscopy (risk of damage)
- Biopsies (same)
Maybe sack your medical team again & eat properly?
Bryan Johnson@bryan_johnson
Bad news #1: I have an autoimmune disease. My stomach is eating itself. Bad news #2: 2–5% of people have this, too. Likely more, because it hides. Good news: I'm going to try and solve it. Will share all. As a kid, I ate sugar cereal, drank sugary soda, and gobbled down fast food. I had a few healthy years in my early 20s but then became a young father of three and began building a business. Juggling that stress and grind, I let my health slip and gained 40 lbs. Within a few years I’d fallen into a deep, chronic depression. Somewhere in that timeline, my body began developing an autoimmune process affecting my thyroid and then my stomach lining. It’s called Autoimmune Gastritis (AIG). My hypothyroidism got diagnosed when I was 21 years old with a routine blood draw. That enabled me to begin proactive management, supplementing levothyroxine and Armour Thyroid. They are the hormones my body should be producing on its own but wasn’t. By taking these pills daily, my body was able to operate as though my thyroid was functioning properly. What I didn’t know was that something else was going on inside my body: my stomach had begun attacking itself. But there was no routine test to find out and I didn’t have any symptoms. I just discovered it in May. I'm unsure how long I've had it. AIG causes irreversible damage: nutritional deficiency, anemia, and over a long horizon, elevated cancer risk. When AIG is discovered today, standard medical care concedes defeat, stating that nothing can be done except managing the condition, no matter how awful or lethal the effects. Looking back over the past few years, I can now see the early signals we were picking up in measurement but hadn’t connected the dots. For 11 years, I’ve had low ferritin, without anemia. We continually tried to raise my iron levels with food and supplementation but nothing would work. We chased the obvious solutions first. A plant-based diet means all my iron is the hard-to-absorb, non-heme kind. Hard training, sauna, and hyperbaric oxygen all raise the body's demand for iron. But none of them explained the core failure: despite me taking iron orally, trialing every formulation, and using every timing trick, none of the iron would stick. What I didn’t fully appreciate until recently is how many stones my previous providers had left unturned. The low ferritin kept getting explained away but not fixed. I overhauled my medical team earlier this year. It was the rebuild to lay the groundwork for Immortals Care, our $1M a year protocol. With greater capacity, we revisited everything. On the surface, my low ferritin was easy to dismiss by most standards of care. My hemoglobin and hematocrit were normal. Ferritin measures stored iron, while hemoglobin measures circulating iron, and because the body drains its reserves first to keep hemoglobin normal, you can be fully iron deficient with a perfectly normal hemoglobin and hematocrit. This is why my low ferritin kept getting dismissed: the numbers that define anemia looked fine, so no one asked why my iron reserves wouldn't refill. My team pressed on that question. They first turned to a colonoscopy. I was 48 years old and overdue. It was good health hygiene to have while also serving a specific purpose of searching for a hidden source of blood loss such as a polyp or even cancer in my bowels. Either one of those would be an explanation of why the iron kept disappearing. At the same time, they began connecting the dots. Iron absorption depends on stomach acid, so one theory was that my stomach acid was disrupted. They also knew that thyroid and stomach autoimmunity often travel together, so often that the pairing has a name: thyrogastric syndrome. Put against my 27+ year history of autoimmune thyroid disease, the pieces pointed to a single hypothesis: my own immune system was attacking my stomach. To our surprise, my colonoscopy came back clean. A perfectly healthy colon, better than 95% of colonoscopies of men, according to the gastroenterologist. That ruled out the first concern and worst possible outcome: slow continuous bleeding from colon cancer, or pre-cancerous polyp. My team had exercised great foresight though, anticipating this possible outcome. In addition to a colonoscopy, they’d ordered an upper endoscopy to be performed at the same time. The combined procedure is a bi-directional endoscopy. Probes would look at my entire intestinal tract, up from below and down the throat. Additionally, we had several blood biomarkers measured ahead of the procedure to try and pick up on any signals that would give the gastroenterologist guidance for what to look for while doing visual inspections. Fifteen minutes before the procedure, my blood results returned, finding elevated levels of anti-parietal-cells-antibodies (APCA). They came back at roughly five times the upper limit of normal (103, against a ceiling of 20 Units/mL). It was a positive result confirming the suspicion of AIG being the culprit behind my low ferritin, the other type of gastritis, driven by a bacterial infection, was already ruled out, as we knew I am negative to H. pylori. Even before this finding, my team had ordered five biopsies to be taken from three regions of my stomach. The biopsies were the critical piece. Had they not been ordered, the bi-directional endoscopy would have been completed and AIG remained undiagnosed as there were no visual signatures of the condition in my intestines. Two days later, the results of biopsies came in, showing clear signs of early autoimmune gastritis: early atrophy confined to the acid-producing lining, with the rest of the stomach still spared. My team had anticipated this, methodically tracing every line of evidence. We now had a formal diagnosis. I have autoimmune gastritis AIG. My stomach is eating itself. So this was never one problem. It was three, linked to one another: the iron deficiency, the autoimmune gastritis driving it, and the autoimmune thyroid disease alongside it. Iron and thyroid feed each other both ways, low iron impairs the conversion of thyroid hormone into its active form, and an under active thyroid impairs how the body uses iron. Each made the other harder to fix. Autoimmune gastritis affects an estimated 2–5% of people, and likely more, because it hides and is challenging to diagnose. It's usually silent for years, surfacing only once the stomach has atrophied enough to do real damage: iron deficiency first, then B12 deficiency, then anemia from both, and over a long horizon, raised stomach-cancer risk. In one study of people with precancerous gastric lesions, roughly 18% carried the autoimmune antibodies, and only about 1% had ever been diagnosed. And the earliest clue, low ferritin, is the one standard medicine waves through. Low iron stores get normalized and rarely investigated at all when anemia hasn't shown up yet. That blind spot is what hid mine for a decade. The good news: the iron deficiency is now corrected. I received a 1,000 mg Monoferric iron infusion. This was chosen for two reasons after considering multiple formulations. First, it can safely deliver a full dose of iron in a single infusion (1,000 mg), while older options like Venofer require several separate appointments to reach the same total. Second, certain other IV iron formulations can cause a drop in blood phosphate levels, an important mineral for bones and energy. Monoferric is much less likely to do this, which matters given how closely we track long-term metabolic and bone health parameters. As mentioned earlier, current medical standards treat AIG as something to be managed, not resolved. It's worth noting that many of you give me a hard time, inviting me to "live life" and engage in self-destructive behaviors like a "normal person". I'm cool with the playful ribbing. Also, had I not taken care of my health during the past five years, my situation could potentially be very serious. You too may have a lurking health issue that is undiagnosed and could increase in severity from unhealthy life choices, without your knowing. The absence of symptoms is not the presence of health. A gentle nudge that minding your health, no matter your situation in life, is good decision making. My team and I are going to try and solve my AIG. This is how we’re approaching it: First, routine monitoring keeps the disease in view: ferritin and iron, B12, the pepsinogen I/II ratio, gastrin, and chromogranin A. Gastrin is the dial to watch. If it climbs, the disease is advancing, and the risk of gastric neuroendocrine tumors climbs with it. Second, we’re doing advanced characterization of the disease. We’ll do a repeat biopsy to read the immune infiltrate, deep cytokine profiling, and T-cell subset analysis, to see which pathways are actually firing. That testing drives the intervention plan, including the experimental approaches we intend to develop. + If gastrin and chromogranin rise: damp the gastrin drive (netazepide) and tighten endoscopic surveillance. If the profile is Th1 / interferon-driven: target JAK/STAT. + If it's Th17 / IL-17-driven: target IL-17 and STAT3. + If regulatory T cells are failing: rebuild them (low-dose IL-2, induced Tregs). + If it's antibody- and B-cell-driven and antigen-specific: engineered cell therapy (CAAR-T). Which organizes into four tiers, from available today to frontier: Tier 1, now: protect and support; zinc-L-carnosine, and acid replacement (betaine HCl with pepsin) under physician supervision. This is specific to my case and not something to self-prescribe, especially given the cancer-surveillance considerations above. Tier 2, target the signaling , JAK/STAT, GSK-3, IL-17, and damp the gastrin drive (netazepide). Tier 3, reset the cells, induced regulatory T cells (iTregs). Tier 4, frontier: engineered T-cell therapy (CAR-T / CAAR-T), custom AI-designed antibodies, or synthetic proteins, that can specifically seek out inactivate or destroy the rogue immune cells attacking my stomach lining. To be clear: there's no approved cure for autoimmune gastritis today. Medicine treats it as something to manage, not solve. Tiers 2 through 4 are investigational preclinical evidence at best, and in several cases therapies that still have to be built. If you're working on autoimmune gastritis, antigen-specific tolerance, regulatory T cells, or CAAR-T for organ-specific autoimmunity, please reach out. Modern medicine has normalized too many conditions that erode our health, function, and comfort, shrinking the goal to monitoring and management while a cure is rarely even attempted. Most of these verdicts were handed down decades ago, in an era that predates nearly all of our current tech and science, and they have gone largely unchallenged. We want to change that. In the age of AI, multiomics, and custom-built DNA, proteins, and cells, no condition should be presumed incurable simply because no one has yet tried to cure it with today's stack. I’ll end on a personal note. We fill our days mostly on things that are trivial next to what we ultimately care about. We know, deep down, however, that in the noise of it all, health is easily forgotten until it’s the only thing that matters. We spend a fraction of our lives truly sober to the preciousness of life. We feel it when someone we love dies, when a child is born, when we come close to death ourselves, or when a diagnosis marks our limit. In those moments, we are sobered, and the rarity of it all becomes self evident. Imagine the existence we’d build together if that clarity didn’t fade. I wish all of you the very best. Care for yourself, care for others, care for the planet and care for our animal friends. Care for life as it’s the most precious gift there is.
English

Elon Musk reveals he caught his doctor trying to scam him with a $1,000 a month supplement and explains how his own blood work exposed the lie
"I went to this doctor who was like highly recommended, you know, doctor to the stars, which is like maybe not a good sign. And he tells me that I'm like B12 deficient. And then he gives me these like B12 supplements and he's going to give me a starter pack. It's going to be like $1,000 a month for these special B12."
Joe Rogan: "$1,000 a month for B12? That's crazy. You get it on Amazon."
Elon Musk: "Yeah, but his one's special. So then I get home, I'm paging through my blood work, and it says I have excess B12. So I'm like, wait a second. And he's giving me pills that have like 20,000% of the recommended daily dose. I took a photograph of the blood work that says I have excess, above the recommended range of B12."
English
@ChrisMasterjohn simply, Vegan isn't the way. Nor is filtering your blood through bizarre and archaic plastic tubes
English

Bryan Johnson has been diagnosed with a disease that mostly occurs in the elderly.

Bryan Johnson@bryan_johnson
Bad news #1: I have an autoimmune disease. My stomach is eating itself. Bad news #2: 2–5% of people have this, too. Likely more, because it hides. Good news: I'm going to try and solve it. Will share all. As a kid, I ate sugar cereal, drank sugary soda, and gobbled down fast food. I had a few healthy years in my early 20s but then became a young father of three and began building a business. Juggling that stress and grind, I let my health slip and gained 40 lbs. Within a few years I’d fallen into a deep, chronic depression. Somewhere in that timeline, my body began developing an autoimmune process affecting my thyroid and then my stomach lining. It’s called Autoimmune Gastritis (AIG). My hypothyroidism got diagnosed when I was 21 years old with a routine blood draw. That enabled me to begin proactive management, supplementing levothyroxine and Armour Thyroid. They are the hormones my body should be producing on its own but wasn’t. By taking these pills daily, my body was able to operate as though my thyroid was functioning properly. What I didn’t know was that something else was going on inside my body: my stomach had begun attacking itself. But there was no routine test to find out and I didn’t have any symptoms. I just discovered it in May. I'm unsure how long I've had it. AIG causes irreversible damage: nutritional deficiency, anemia, and over a long horizon, elevated cancer risk. When AIG is discovered today, standard medical care concedes defeat, stating that nothing can be done except managing the condition, no matter how awful or lethal the effects. Looking back over the past few years, I can now see the early signals we were picking up in measurement but hadn’t connected the dots. For 11 years, I’ve had low ferritin, without anemia. We continually tried to raise my iron levels with food and supplementation but nothing would work. We chased the obvious solutions first. A plant-based diet means all my iron is the hard-to-absorb, non-heme kind. Hard training, sauna, and hyperbaric oxygen all raise the body's demand for iron. But none of them explained the core failure: despite me taking iron orally, trialing every formulation, and using every timing trick, none of the iron would stick. What I didn’t fully appreciate until recently is how many stones my previous providers had left unturned. The low ferritin kept getting explained away but not fixed. I overhauled my medical team earlier this year. It was the rebuild to lay the groundwork for Immortals Care, our $1M a year protocol. With greater capacity, we revisited everything. On the surface, my low ferritin was easy to dismiss by most standards of care. My hemoglobin and hematocrit were normal. Ferritin measures stored iron, while hemoglobin measures circulating iron, and because the body drains its reserves first to keep hemoglobin normal, you can be fully iron deficient with a perfectly normal hemoglobin and hematocrit. This is why my low ferritin kept getting dismissed: the numbers that define anemia looked fine, so no one asked why my iron reserves wouldn't refill. My team pressed on that question. They first turned to a colonoscopy. I was 48 years old and overdue. It was good health hygiene to have while also serving a specific purpose of searching for a hidden source of blood loss such as a polyp or even cancer in my bowels. Either one of those would be an explanation of why the iron kept disappearing. At the same time, they began connecting the dots. Iron absorption depends on stomach acid, so one theory was that my stomach acid was disrupted. They also knew that thyroid and stomach autoimmunity often travel together, so often that the pairing has a name: thyrogastric syndrome. Put against my 27+ year history of autoimmune thyroid disease, the pieces pointed to a single hypothesis: my own immune system was attacking my stomach. To our surprise, my colonoscopy came back clean. A perfectly healthy colon, better than 95% of colonoscopies of men, according to the gastroenterologist. That ruled out the first concern and worst possible outcome: slow continuous bleeding from colon cancer, or pre-cancerous polyp. My team had exercised great foresight though, anticipating this possible outcome. In addition to a colonoscopy, they’d ordered an upper endoscopy to be performed at the same time. The combined procedure is a bi-directional endoscopy. Probes would look at my entire intestinal tract, up from below and down the throat. Additionally, we had several blood biomarkers measured ahead of the procedure to try and pick up on any signals that would give the gastroenterologist guidance for what to look for while doing visual inspections. Fifteen minutes before the procedure, my blood results returned, finding elevated levels of anti-parietal-cells-antibodies (APCA). They came back at roughly five times the upper limit of normal (103, against a ceiling of 20 Units/mL). It was a positive result confirming the suspicion of AIG being the culprit behind my low ferritin, the other type of gastritis, driven by a bacterial infection, was already ruled out, as we knew I am negative to H. pylori. Even before this finding, my team had ordered five biopsies to be taken from three regions of my stomach. The biopsies were the critical piece. Had they not been ordered, the bi-directional endoscopy would have been completed and AIG remained undiagnosed as there were no visual signatures of the condition in my intestines. Two days later, the results of biopsies came in, showing clear signs of early autoimmune gastritis: early atrophy confined to the acid-producing lining, with the rest of the stomach still spared. My team had anticipated this, methodically tracing every line of evidence. We now had a formal diagnosis. I have autoimmune gastritis AIG. My stomach is eating itself. So this was never one problem. It was three, linked to one another: the iron deficiency, the autoimmune gastritis driving it, and the autoimmune thyroid disease alongside it. Iron and thyroid feed each other both ways, low iron impairs the conversion of thyroid hormone into its active form, and an under active thyroid impairs how the body uses iron. Each made the other harder to fix. Autoimmune gastritis affects an estimated 2–5% of people, and likely more, because it hides and is challenging to diagnose. It's usually silent for years, surfacing only once the stomach has atrophied enough to do real damage: iron deficiency first, then B12 deficiency, then anemia from both, and over a long horizon, raised stomach-cancer risk. In one study of people with precancerous gastric lesions, roughly 18% carried the autoimmune antibodies, and only about 1% had ever been diagnosed. And the earliest clue, low ferritin, is the one standard medicine waves through. Low iron stores get normalized and rarely investigated at all when anemia hasn't shown up yet. That blind spot is what hid mine for a decade. The good news: the iron deficiency is now corrected. I received a 1,000 mg Monoferric iron infusion. This was chosen for two reasons after considering multiple formulations. First, it can safely deliver a full dose of iron in a single infusion (1,000 mg), while older options like Venofer require several separate appointments to reach the same total. Second, certain other IV iron formulations can cause a drop in blood phosphate levels, an important mineral for bones and energy. Monoferric is much less likely to do this, which matters given how closely we track long-term metabolic and bone health parameters. As mentioned earlier, current medical standards treat AIG as something to be managed, not resolved. It's worth noting that many of you give me a hard time, inviting me to "live life" and engage in self-destructive behaviors like a "normal person". I'm cool with the playful ribbing. Also, had I not taken care of my health during the past five years, my situation could potentially be very serious. You too may have a lurking health issue that is undiagnosed and could increase in severity from unhealthy life choices, without your knowing. The absence of symptoms is not the presence of health. A gentle nudge that minding your health, no matter your situation in life, is good decision making. My team and I are going to try and solve my AIG. This is how we’re approaching it: First, routine monitoring keeps the disease in view: ferritin and iron, B12, the pepsinogen I/II ratio, gastrin, and chromogranin A. Gastrin is the dial to watch. If it climbs, the disease is advancing, and the risk of gastric neuroendocrine tumors climbs with it. Second, we’re doing advanced characterization of the disease. We’ll do a repeat biopsy to read the immune infiltrate, deep cytokine profiling, and T-cell subset analysis, to see which pathways are actually firing. That testing drives the intervention plan, including the experimental approaches we intend to develop. + If gastrin and chromogranin rise: damp the gastrin drive (netazepide) and tighten endoscopic surveillance. If the profile is Th1 / interferon-driven: target JAK/STAT. + If it's Th17 / IL-17-driven: target IL-17 and STAT3. + If regulatory T cells are failing: rebuild them (low-dose IL-2, induced Tregs). + If it's antibody- and B-cell-driven and antigen-specific: engineered cell therapy (CAAR-T). Which organizes into four tiers, from available today to frontier: Tier 1, now: protect and support; zinc-L-carnosine, and acid replacement (betaine HCl with pepsin) under physician supervision. This is specific to my case and not something to self-prescribe, especially given the cancer-surveillance considerations above. Tier 2, target the signaling , JAK/STAT, GSK-3, IL-17, and damp the gastrin drive (netazepide). Tier 3, reset the cells, induced regulatory T cells (iTregs). Tier 4, frontier: engineered T-cell therapy (CAR-T / CAAR-T), custom AI-designed antibodies, or synthetic proteins, that can specifically seek out inactivate or destroy the rogue immune cells attacking my stomach lining. To be clear: there's no approved cure for autoimmune gastritis today. Medicine treats it as something to manage, not solve. Tiers 2 through 4 are investigational preclinical evidence at best, and in several cases therapies that still have to be built. If you're working on autoimmune gastritis, antigen-specific tolerance, regulatory T cells, or CAAR-T for organ-specific autoimmunity, please reach out. Modern medicine has normalized too many conditions that erode our health, function, and comfort, shrinking the goal to monitoring and management while a cure is rarely even attempted. Most of these verdicts were handed down decades ago, in an era that predates nearly all of our current tech and science, and they have gone largely unchallenged. We want to change that. In the age of AI, multiomics, and custom-built DNA, proteins, and cells, no condition should be presumed incurable simply because no one has yet tried to cure it with today's stack. I’ll end on a personal note. We fill our days mostly on things that are trivial next to what we ultimately care about. We know, deep down, however, that in the noise of it all, health is easily forgotten until it’s the only thing that matters. We spend a fraction of our lives truly sober to the preciousness of life. We feel it when someone we love dies, when a child is born, when we come close to death ourselves, or when a diagnosis marks our limit. In those moments, we are sobered, and the rarity of it all becomes self evident. Imagine the existence we’d build together if that clarity didn’t fade. I wish all of you the very best. Care for yourself, care for others, care for the planet and care for our animal friends. Care for life as it’s the most precious gift there is.
English
@BrianAtlas Genocide is corporate sponsored, at every stage of the corporate ladder and through their marketing strategies of course.
Let's face it, Global Mouse Utopia is really hot right now 😂 nothing can stop it
English

This is misandrist Jackie Marie Smith. She has a blue check on TikTok, nearly 1M followers, is sponsored by dozens of MAJOR brands, and is repped by CAA (the biggest talent agency in the world). If a man was putting out this sort of sexist rhetoric about women he would be cancelled, banned off TikTok, and dropped by CAA/sponsors. We truly must start scrutinizing the femisphere and the acceptance & tolerance of anti-male sexism. For now, I call on CAA to drop her as they would drop a male talent espousing anti-woman rhetoric. These are the brands she has worked with just in the past year: @Target, @Amazon, @Walmart, @OldNavy, @Dove, @ultabeauty, @blueapron, @Clinique, @v8energy, @Covergirl, @BurtsBees, @skims, and many more.
English
@photobiogenesis That's cool but if you don't like aging as fast as boomers, you want the minimum healthy amount of iron, to reduce free iron oxidative effects including AGEs & ALEs.
Eating dairy products (calcium) with red meat are more effective than polyphenols to reduce heme iron absorption
English

Oysters are to zinc what red meat is to iron
70% of iron in red meat is encased with a porphyrin ring structured called heme, while the remaining 30% is a mix of soluble/insoluble
Heme utilizes separate absorption channels so it does not compete with other minerals like zinc and calcium for absorption
It has 2-3x higher bioavailability than non-heme iron
Oysters contain a variety of tripeptides and other small peptides which bind zinc, and in this form zinc is taken up through food peptide channels like PEPT1
Peptides-bound zinc also is not bound anti-nutrients like phytates
Because of this zinc from oysters is also 2-3x more bioavailable than supplements sources, which have extremely low bioavailability ranging from 1-9%

English
@chrismartenson @Matt_Bracken48 Commodities reacting to a zombie, outsourced economy, a leading indicator of equity bubble popping soon. Buy the dip in commodities ahead of the AI fire sale
English
By this fall, I may have to reevaluate everything I thought I knew about how the world works.
If nothing we anticipated actually happens by September, it’s time to rethink everything. Oil reality vs. falling prices, SPR being drained to decade lows while inventories crash, COVID/Fauci lessons on how deep the deception goes, markets living in pure narrative… something’s really off.
Full report for Peak members: peakprosperity.pulse.ly/mjcsdmhv9i
What am I missing? Time to rethink? Drop your thoughts.
English
@bryan_johnson Somebody living rent free in Bryan's high pressure hyperbaric head lol
English
Nassim has been pretty tough on me, saying
"the contempt...disgust I have for your brand of non-stoical neurotic overoptimization."
But you know what, I really like Nassim. His books are great, his perspectives are unique, and I enjoy how he thinks.
Nassim Nicholas Taleb@nntaleb
The problem with @bryan_johnson is attribution: we’ll never know which drug, or combination of drugs, did him in.
English
If you are buying Smart Water with your hard-earned dollars, it's not working...

English