Daniel Tawfik@dantawfik
The relationship between sleep duration and biological aging just got mapped across nine organ systems—and the pattern is remarkably consistent.
A new Nature study analyzed 23 biological aging clocks derived from brain imaging, plasma proteomics, and metabolomics across 500,000 individuals in the UK Biobank. The goal was to determine whether sleep duration shows a systematic relationship with biological age across multiple organs and molecular layers—not just the brain.
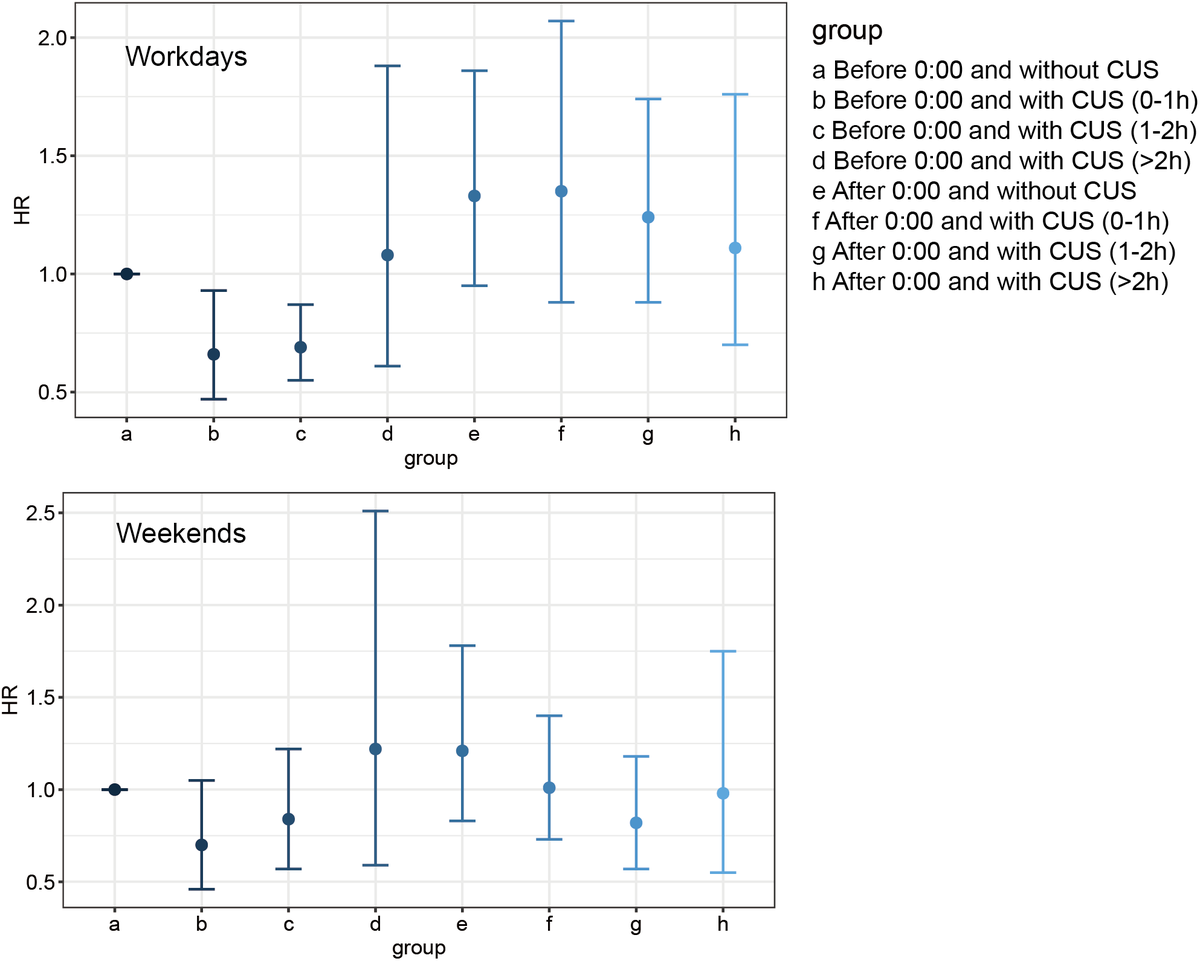
The result: a U-shaped curve appears across nearly every system measured. Both short sleep (under 6 hours) and long sleep (over 8 hours) are associated with accelerated biological aging compared to the optimal range.
The sample-specific minimum biological age gap—the point where aging appeared slowest—occurred between 6.4 and 7.8 hours of sleep per night. That range varied slightly by organ system and sex, but the pattern held across brain structures, metabolic markers, and protein profiles.
This isn't a single biomarker showing correlation. It's a cross-organ, multi-omics signal suggesting that sleep duration operates as a systemic regulator of biological aging—not just a neurological phenomenon.
The study used generalized additive models to fit the nonlinear relationship without assuming a specific curve shape. The U-shaped pattern emerged independently across imaging-derived aging clocks (MRIBAG), proteomic clocks (ProtBAG), and metabolomic clocks (MetBAG).
That consistency across measurement modalities reduces the likelihood that the signal reflects methodological artifact. When three independent molecular and structural aging measures converge on the same sleep duration range, it suggests an underlying biological relationship.
Beyond aging biomarkers, the study linked short and long sleep duration to increased risk of systemic diseases: depression, diabetes, ischemic heart disease, and all-cause mortality. Genetic correlation analyses confirmed associations with 527 disease endpoints across multiple organ systems.
The distinction between short and long sleep matters. The mechanisms appear different.
Short sleep duration showed a more direct association with late-life depression—suggesting that insufficient sleep may produce psychiatric risk through pathways independent of accelerated biological aging.
Long sleep duration, by contrast, showed evidence that biological aging clocks partially mediate the pathway to depression. That pattern suggests chronic long sleep may reflect or drive aging processes that then increase vulnerability to mood disorders.
The study used Mendelian randomization to test whether diseases causally affect sleep duration. The evidence was weak—suggesting that while disease might influence sleep, the primary direction appears to flow from sleep patterns to health outcomes rather than the reverse.
That directionality matters clinically. If sleep duration were primarily a consequence of disease burden, optimizing it would have limited preventive value. But if sleep operates as a modifiable upstream factor—one that influences biological aging across systems—then interventions targeting sleep architecture could alter disease trajectories.
The sample-specific optimal range of 6.4 to 7.8 hours is narrower than the broad 7-9 hour recommendation typically cited. Individual variation exists, but the data suggest that consistently sleeping outside this range—whether above or below—compounds biological aging year over year.
This shifts the framing of sleep optimization from subjective well-being to quantifiable aging deceleration. The decisions about whether to prioritize sleep duration in the fourth and fifth decades may determine the biological age of organ systems in the seventh and eighth.
The relationship isn't linear. Sleeping 5 hours doesn't just subtract proportionally from health compared to 7 hours—it crosses a threshold where multiple aging systems begin accelerating simultaneously. The same appears true beyond 8 hours.
That threshold effect means interventions should target the optimal range, not simply more sleep. Chronic long sleep duration may signal underlying pathology or may itself contribute to metabolic and cognitive decline through reduced circadian stimulus and decreased time spent in metabolically active states.
One limitation: the study relied on self-reported sleep duration. Self-report captures different aspects of sleep than actigraphy or polysomnography—it reflects perceived sleep rather than objective architecture. The correlation between modalities is only moderate.
But the sample size of 500,000 compensates for measurement noise. Even with imperfect individual-level data, population-level patterns emerge robustly when the signal is consistent across organ systems and molecular layers.
The practical implication: sleep duration operates as a systemic aging regulator that can be measured, tracked, and potentially modified before clinical disease manifests. Most aging interventions target downstream pathways—inflammation, oxidative stress, mitochondrial function. Sleep duration may modulate all three simultaneously through a single behavioral variable.
The question isn't whether sleep matters for aging. The question is whether optimizing sleep duration within the 6.4-7.8 hour range can measurably slow multi-organ biological aging and reduce systemic disease risk across decades.
This study suggests the answer is yes.