
Amith Reddy Seri
57 posts
Amith Reddy Seri
@amithseri
Hospitalist @WVUPrinceton | Research Collaborator @MayoclinicAZ | Cardiology Aspirant | Osmania Medical College Alum | @LFHS Alum
Michigan, USA Katılım Mart 2016
257 Takip Edilen142 Takipçiler

JAMA Cardiology is seeking early-career cardiologists or researchers looking to gain hands-on training in the editorial and peer-review processes of an international leading medical journal.
🔗 Learn more and apply here: ja.ma/41PpRA3
English
Amith Reddy Seri retweetledi

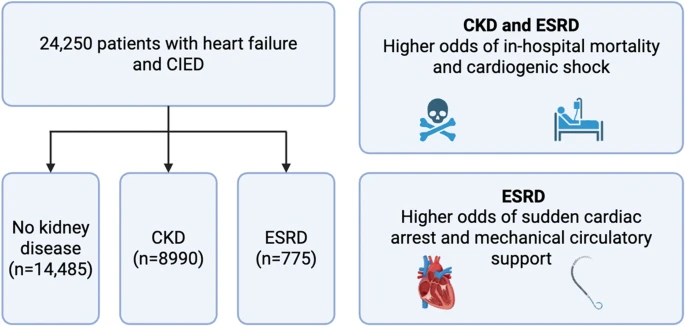
🎉 Congratulations to @amithseri and team for publishing their original research in @JICE_EP under the mentorship of @chadialraies.
“Impact of Underlying Kidney Disease on the Outcomes of Cardiac Implantable Electronic Devices in Patients With Heart Failure”
English
Honored to officially become a Fellow of the American College of Cardiology at the 75th Convocation ceremony! @ACCinTouch

English
Amith Reddy Seri retweetledi

Here’s a sign to meet your long distance medschool besties because what do you mean you were the same people who cried blood tears the night before Surgery paper 2 few years ago, but now here you are (whispering)*real doctors* & all that.

English
Amith Reddy Seri retweetledi

Just published 🚨🚨
Levosimendan improved some outcomes in advanced HF:
🟩⬆️ LVEF
🟩⬇️ All-cause Mortality
🟩⬇️ BNP
⬛⬛ No effect on HF Rehospitalization
More details on American Journal of Cardiovascular Drugs:
link.springer.com/article/10.100…

English

Updated GI Fellow Resources
If you have not already downloaded this app from @EmoryGastroHep, I highly recommend it!
It’s been added to the hyperlinked-PDF below.
📲 bit.ly/3KwqCVG (hyperlinked 📄)

Emory Gastroenterology and Hepatology Fellowship@EmoryGastroHep
🔥🔥Emoroid Digest🔥🔥 The moment you have been waiting for… THE EMOROID DIGEST APP!!! Get our content on the go on your mobile devices & help deliver evidence based care to your patients!! Download for FREE now on Apple Store or Google Play! See ⬇️ for links!
English
Amith Reddy Seri retweetledi

We propose that a "Heart Failure Internist" is an internal medicine physician who completed additional comprehensive HF training. We further propose that by further diversifying the HF clinical workforce with these unique specialists we will be able to provide more and better care. Multiple such fellowships already exist in the US, and there is a rising interest from more institutions.
Below is the full text of our Leading Edge Commentary published in #JACCHF @JACCJournals. Thank you to Editors @BiykemB and @MinnowWalsh for being open to publishing on this controversial topic. Kudos to my co-authors Drs. Brett Sperry and Andrew Lenneman, who are also Program Directors of these programs in their respective institutions. And thank you to the @HFSA, who recently expanded HF-Cert eligibility to graduates of these training programs.
Heart Failure Training for the Internist: A Potential Solution for the Heart Failure Workforce Shortage
There are insufficient numbers of trained clinicians to meet the demands of the heart failure (HF) epidemic in the United States. Although multiple strategies are being evaluated to meet these needs, we focus on an underappreciated but growing pathway to obtain HF training: the HF Internist.
The Problem
The burden of HF in the United States is massive and growing. Per published American Heart Association statistics, it is anticipated that >8.5 million adults will be affected by 2030.4 Further, HF diagnostic and therapeutic modalities have become increasingly more complex and involve multiple stakeholders. In the context of this increased complexity, it is perhaps not surprising that HF care is often suboptimal with multiple registries describing underdiagnosis of cardiomyopathies, underutilization of guideline-directed medical therapy and appropriate implantation of devices, underrecognition and under management of cardiac resynchronization therapy nonresponse, and significant under-referral of patients with Stage D HF for advanced therapy evaluations.
In 2009, the ABIM (American Board of Internal Medicine) certified subspecialty training programs in advanced heart failure and transplant cardiology (AHFTC) to be completed after cardiology fellowship. Before this, several programs offered advanced training that focused on transplant cardiology and the burgeoning field of mechanical circulatory support (MCS). This training was primarily done at transplant centers, usually for an additional year before or after fellowship training in cardiovascular disease. Many of those trained in this way elected to take the ABIM AHFTC board exam when it became available. Now, ∼1,400 cardiologists are board certified in this discipline. Training in AHFTC continues to be focused typically on transplantation and MCS, and the job market for these positions is stagnant as expansion of transplant/MCS has not risen concomitantly with the rate of graduating fellows. This, among other reasons, has led to a declining interest in subspecialty AHFTC training among general cardiology trainees, and between 55% and 60% of fellowship positions have gone unmatched in the United States over the 2020-2023 cycles. In practice, internists, hospitalists, and primary care physicians care for the largest number of patients with HF. Among cardiologists, general cardiologists are the primary workforce caring for the HF population, but there are only modest COCATS (Core Cardiology Training Symposium) requirements for dedicated HF content in general cardiology training and >40% of U.S. cardiology fellowship programs do not have an AHFTC-trained specialist on staff.
Although there is important ongoing work to increase the HF clinical workforce, including investigating ways to improve the value of AHFTC training, elevating expertise among general cardiologists, and recruiting and training more HF-focused advanced practice providers, little attention has been paid to training an entirely novel HF workforce: the HF internist.
The HF Internist
We propose that an HF internist is an internal medicine (IM) residency graduate who completed additional comprehensive HF training under mentorship of experienced AHFTC subspecialty cardiologists and their colleagues. Multiple programs in the United States currently offer such training, most commonly referred to as a “non-accredited heart failure fellowship.” The goal of these HF fellowship programs is to provide comprehensive training in the care of patients with HF. The demand for this training is high, and is primarily driven by IM residency graduates who failed to match into cardiovascular disease fellowships and who desire additional training as a steppingstone to matching. Other pathways pursued as a means for applicants to strengthen their candidacy include research, hospitalist positions, and other nonaccredited fellowships such as advanced cardiac imaging, hypertension, preventive cardiology, and vascular medicine, among others. Competition for accredited cardiovascular disease training spots is high with only 2 of every 3 candidates matching, leaving behind many candidates who go unmatched.10 The profile of these applicants is diverse and includes graduates of community-based IM programs in which more complex cardiac training was lacking, international and osteopathic medical school graduates who historically have had a harder time matching into cardiology, and hospitalists. In addition, some prospective cardiology fellows realize that their applications need to be strengthened, so taking an extra year of cardiac subspecialty training shows dedication to the field and allows for additional clinical and research experience before applying for fellowship.
If the HF internist ultimately matches into cardiology fellowship, they will enter with a unique skillset that could be built on to launch a career as a general cardiologist with a focus in general HF, an area with immense need. Although completing HF internist training as described here anecdotally appears to increase the probability of trainees matching, it does not universally result in match success. Regardless, the HF-related expertise that these trainees acquire is carried forward into a variety of other careers. Focused HF training may result in improved patient outcomes through patient-centered coordination of multidisciplinary care and increased utilization of guideline-directed medical therapy.
Outside of cardiology, graduates from our programs have gone on to become hospitalists, nephrologists, critical care specialists, and geriatricians—all areas in which additional HF expertise is immediately relevant and valuable. In either case, we feel that additional training in HF should be encouraged and validated by professional societies in an effort to increase the workforce of physicians with expertise in HF.
Training Content and Certification
Content of the 12-month training program for the HF internist would be focused on general HF care. Given the understanding that many internists seeking out this additional training are interested in pursuing an accredited cardiovascular disease fellowship, we advocate for ample flexibility to pursue experiences in other aspects of cardiology as well as research.
In our HF internist training programs we offer approximately 6 months of inpatient rounding on the HF service with a focus on treatment of HF exacerbations, the progression to Stage D HF, and cardiac critical care. Fellows’ roles on these rotations vary and include responsibility for diagnostic and management tasks for patients on the floor, intensive care unit, and in consultative contexts, all under supervision of an AHFTC-trained cardiologist. Approach to overnight call and weekend rounding coverage varies among programs. Training programs that require overnight and weekend service should adhere to accepted ACGME (Accreditation Council for Graduate Medical Education) work-hour restrictions. Weekend and overnight moonlighting may also be available. Fellows perform procedures in the catheterization laboratory and intensive care unit (primarily right heart catheterizations). Elective rotations in multimodality cardiovascular imaging are also recommended, with a focus on echocardiography. Palliative medicine experience is strongly encouraged/required. We also offer exposure to the outpatient HF clinic, as well as outpatient HF-related subspecialty clinics (adult congenital, amyloid, cardiometabolic, cardio-oncology, CRT nonresponder, hypertrophic cardiomyopathy, pulmonary hypertension, palliative care, and valve). Quality improvement or clinical research is encouraged, and appropriate mentorship is provided. These experiences are under the direction of an AHFTC-certified team of cardiologists.
For any training program to thrive, acceptance from professional societies and a path toward certification is needed. The HFSA (Heart Failure Society of America) currently has an HF certification program (HF-Cert) geared toward experienced health care providers (physicians, pharmacists, advanced practice providers, and nurses) to recognize them with the advanced-level knowledge and skill to provide competent HF services in the United States. Eligibility requires an advanced degree and at least 3 years of experience (1,240 hours) with a practice focus in HF. Although graduates of HF internist fellowships were previously not eligible to sit for the exam, HFSA’s HF-Cert Council recently decided to change this. Effective in 2024, eligibility for HF-Cert will be expanded to include “physicians who have completed a dedicated 1-year nonaccredited heart failure fellowship and meet the experience hours requirement.” Applicants will need to provide a letter from their fellowship’s program director attesting completion of the required 1,240 hours of clinical HF experience. We feel that this is important progress in recognizing both the value of these clinicians, and the HF internist model.
Challenges and Criticisms
Several challenges and criticisms must be recognized in this discussion of the HF internist model.
First, the concept of training IM graduates in HF fellowships is not new. Before ABIM certification of AHFTC training as it exists now, a variety of HF training programs existed, many of which also trained IM graduates. What was lacking then across programs was what we propose in this commentary: development of a standardized milestone-based curriculum that is tailored to noncardiologists. As noted earlier, we believe that this would need to be developed in a future state. Developing such a curriculum would differentiate between HF internist training and ACGME-accredited AHFTC fellowships.
Second, physicians already endure many years of education and training, so adding an additional year after IM residency may be viewed as a burden. Although we are not proposing that an HF-focused year is required to care for patients with HF, we do believe that the additional expertise will be of great benefit to communities/populations of patients. We also want to empower and validate recent graduates and current trainees seeking out this added training.
Third, the exact type of career that the HF internist will pursue after training will be varied. Although some of these graduates will continue to general cardiology training, others will pursue other IM pathways. We believe that over time HF internists can become valuable partners for cardiologists and tertiary advanced HF and transplantation teams. For example, a recent graduate went on to staff a part-time HF clinic in rural Indiana. Another graduate went on to do a geriatrics fellowship, and now uses her combined expertise caring for patients in a community hospital. It is also likely that HF internists will be able to take on important leadership roles in their respective health care systems, in close partnership with cardiologists.
Fourth, funding for a non–ACGME-accredited program typically comes from institutional or grant sources and may be a challenge. With increased validation, recognition, and certification, this may become easier to address in the future.
Fifth, beyond our anecdotal experiences as HF internist fellowship program directors, published data about applicants to HF internist training programs, trainee profiles, and postgraduation trajectories is lacking. We believe that comprehensive surveys of existing programs are an important next step.
Finally, some have expressed concerns that the border between HF internists and specialized advanced HF cardiologists can be blurred, thus creating confusion not only for other providers but for patients. Although we recognize that the long-term impact of HF internists on the HF ecosystem is unknown, we believe that their addition will be complementary, incremental, and additive. The standardized curriculum we propose for HF internist training would focus on the community- and population-based needs of patients with Stage B through D HF, and not on skills related to critical care, catheterization-based procedures, and advanced HF therapies. We strongly believe that forward thinking systems could create hub and spoke models allowing HF internists and advanced HF cardiologists to work together, which would result in multiple wins including better care for populations and simultaneously growing advanced HF therapy volumes.
In summary, we argue for the importance of training additional physicians in care of patients with HF, and propose a framework for the identification, training, and certification of these physicians. Although many strategies should be identified and formalized to improve the care of the ever-increasing population of patients living with HF, we feel that elevating the HF internist is one such approach that should be considered.
jacc.org/doi/full/10.10…
English
Amith Reddy Seri retweetledi

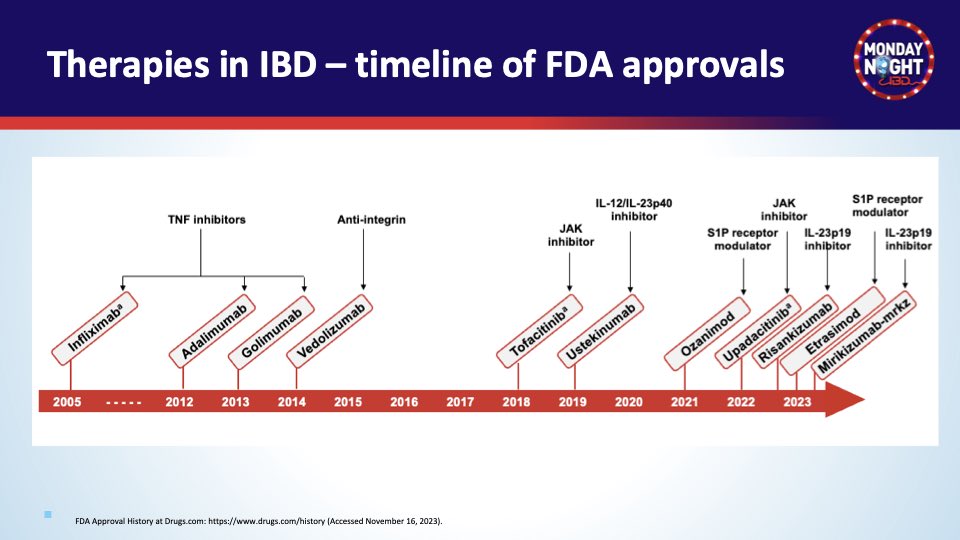
@MondayNightIBD @BassiMehak @abbvie @JanssenUS @TakedaPharma 1/ Welcome #GITwitter #IBDTwitter to another 🔥#MondayNightIBD #Back2Basics. Let’s talk FDA-approved advanced therapies in mod-severe #IBD 👇
🔑Several MOA available! Let’s review: standard dosing, indications, monitoring, SE/Caution, efficacy in bio-naïve/exposed
Kansas City, MO 🇺🇸 English

Introducing The Yearly Review: Your In-Depth Reflection Guide for 2023.
• Reflect on the past year
• Pinpoint what worked & what didn't
• Turn your biggest takeaways into content
Sharing it for free until Friday.
Like & reply "review" and I'll DM it to you!

English
@KeyurBShahRIC @VCUHealthHeart Hi! I am interested. Can you please share the details? Thanks
English

IM PGY-3s and beyond: interested in a cardiology focus? Consider one of our two Heart Failure Scholar positions @VCUHealthHeart Enriched with QI, Scholarly Activities and Clinical preparation. DM me for more information.
Manhattan, NY 🇺🇸 English
Amith Reddy Seri retweetledi
Kudos to Mayo’s Media Team for shining a spotlight on our AugMAP study!
newsnetwork.mayoclinic.org/discussion/may…
AugMAP identifies high-risk patients with moderate aortic stenosis. Let's think beyond routine surveillance and explore alternative management strategies. @MayoClinicCV
#AugMAP #AS
United States 🇺🇸 English
English

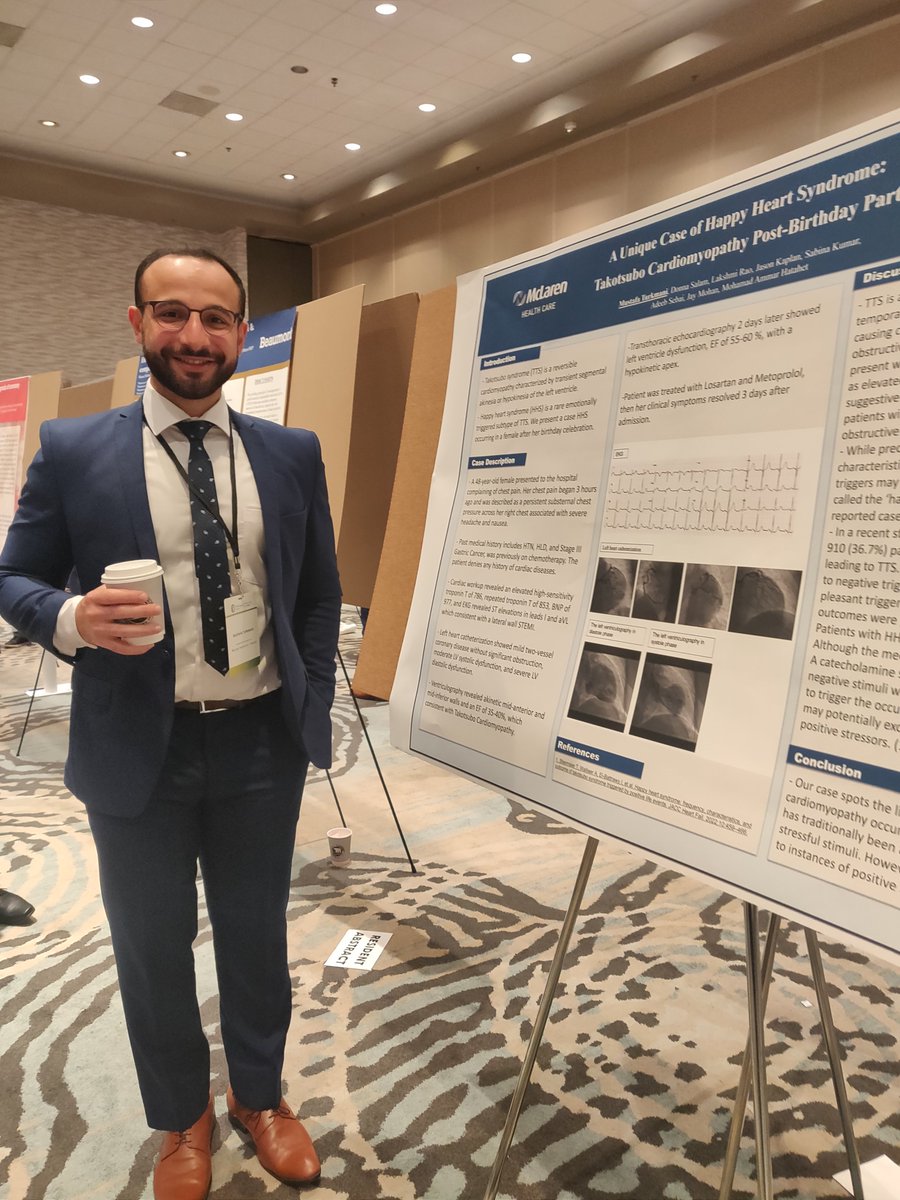
What a beautiful weekend up-north for Michigan ACC! I'm thrilled to share that I've been awarded the title of Top Poster Presentation!!
I'm grateful for the support I've received throughout my journey. I extend my heartfelt thanks to @Babar_Basir& @MichiganACC board! @ACCinTouch


English

Congratulations @amithseri!
Amith Reddy Seri@amithseri
I'm very honored to have been inducted into the prestigious Alpha Omega Alpha (ΑΩΑ) medical honor society. I guess I never have to ✔️"there's no ΑΩΑ in program" when I apply for further fellowships. I'm so thankful to my program for nominating me. @ACCinTouch @MichiganACC
English
I'm very honored to have been inducted into the prestigious Alpha Omega Alpha (ΑΩΑ) medical honor society.
I guess I never have to ✔️"there's no ΑΩΑ in program" when I apply for further fellowships.
I'm so thankful to my program for nominating me. @ACCinTouch @MichiganACC
English
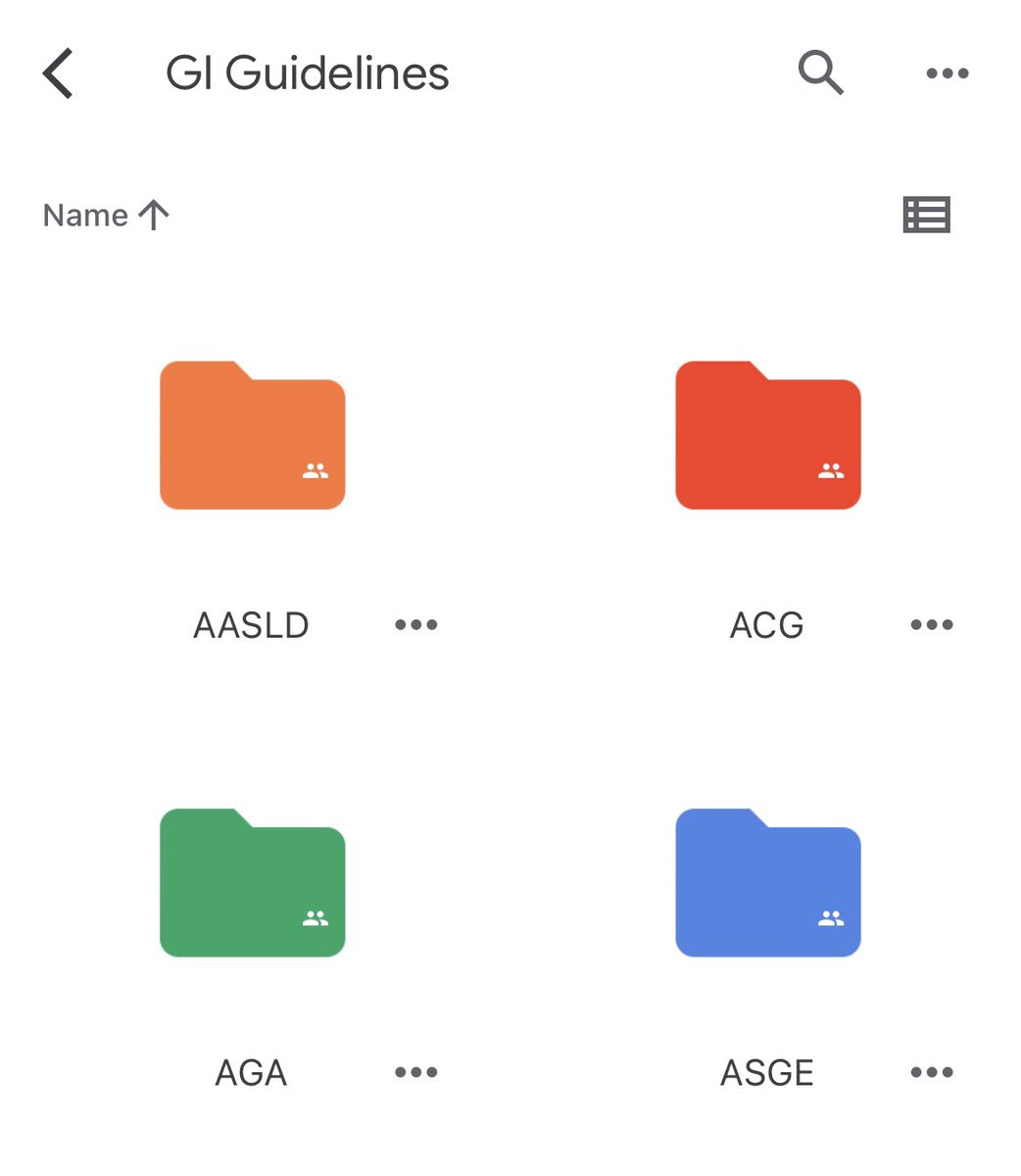
All 4️⃣ GI Society Guidelines in 1️⃣ Place
@AGA_Gastro 48 guidelines
@AmCollegeGastro 55 guidelines
@ASGEendoscopy 83 guidelines
@AASLDtweets 23 guidelines
Google folder:
🔗 drive.google.com/drive/folders/…
Save this link & quickly download all PDFs
Updated as 🆕 guidelines published!
English
Amith Reddy Seri retweetledi
Our paper, "Topological Data Analysis Identified Prognostically-distinct Phenotypes in Transcatheter-Edge-to-Edge Repair Patients," is now published in Mayo Clinic Proceedings: Digital Health 🎉 Read it here: [Link](authors.elsevier.com/sd/article/S29…) @MayoClinicCV #AIInnovation #healthcare
Palo Alto, CA 🇺🇸 English
Hot off the press 🔥
“Adding Pharmacist-Led Home Blood Pressure Telemonitoring to Usual Care for Blood Pressure Control: A Systematic Review and Meta-Analysis” @avolgman @timir_paul @joshmitchellmd
sciencedirect.com/science/articl…
English
Adding pharmacist-led home BP telemonitoring to usual care achieves better BP control than usual care alone.
English