Sabitlenmiş Tweet
Tejaswi Kanala MD
1.2K posts


Tejaswi Kanala MD
@TSKanala
RadOnc | Fellow @MDAndersonNews | @RadOncTMC, OsmaniaMed alum | @CanGenetics_TMC | Organ preservation & Radiobiology | opinions my own |
Houston, TX Katılım Kasım 2018
721 Takip Edilen861 Takipçiler
Tejaswi Kanala MD retweetledi

Interesting that a review on TNT for LARC- w/ extensive discussion of RT toxicity & RT omission - has 0 rad onc authors, cites bowel tox data from 2005, and mischaracterizes PROSPECT data: no better QoL with chemo as they state, but different toxicity profile and no diff in HRQoL
Journal of Clinical Oncology@JCO_ASCO
Disruptive Analysis of Total Neoadjuvant Therapy in Locally Advanced Rectal Cancer: Clinical and Therapeutic Distinctions Between Low- and Mid-Rectal Cancers. Read the full article. ascopubs.org/doi/abs/10.120… #gicsm
English
Tejaswi Kanala MD retweetledi

Paid summer internships at the Dept of Radiation Oncology at Tata Medical Center, Kolkata on a number of projects in AI/ML and bioinformatics.
If you are interested in getting into health applications of AI, this a great opportunity.
DM for more info. #AI #oncology #internship
English
Tejaswi Kanala MD retweetledi

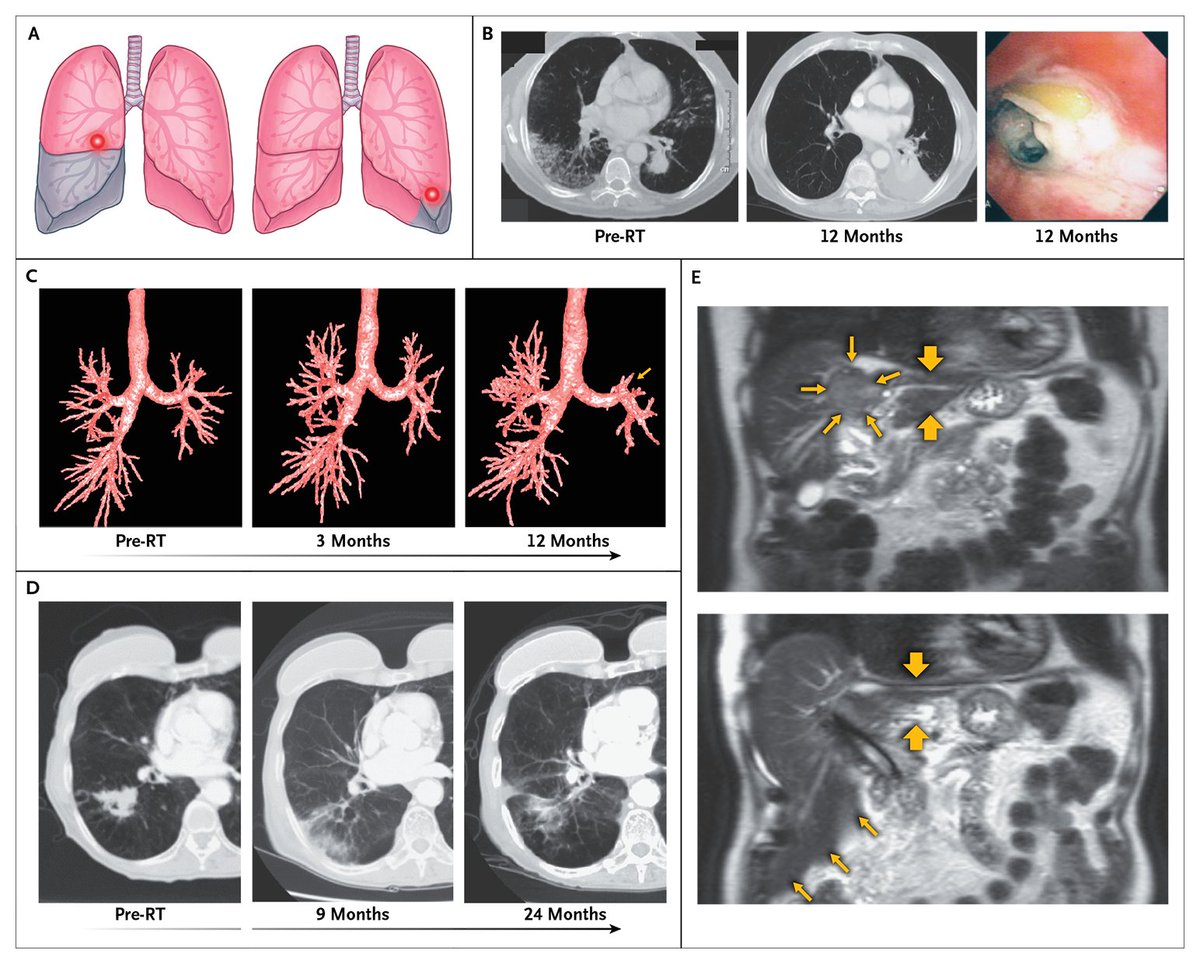
𝗕𝗶𝗼𝗹𝗼𝗴𝗶𝗰 𝗨𝗻𝗱𝗲𝗿𝗽𝗶𝗻𝗻𝗶𝗻𝗴𝘀 𝗼𝗳 𝗦𝗶𝗱𝗲 𝗘𝗳𝗳𝗲𝗰𝘁𝘀 𝗼𝗳 𝗥𝗮𝗱𝗶𝗮𝘁𝗶𝗼𝗻
Radiobiologic models developed with the use of characteristics such as mitotic capacity, tissue hierarchy, and differentiation state can predict responses in normal tissue at the levels of the cell, tissue, and organ. For example, the interaction of the dose and volume of radiation with the risk of effects in normal tissue is tissue- or organ-specific and dependent on the organization of the smallest functional subunits (e.g., nephrons, neurons, or alveoli) within the tissue. For some organs in which the functional subunits are organized in parallel (e.g., nephrons in the kidney), approximately a third of the total volume of the organ must be spared from receiving a relatively low threshold dose to maintain functional organ viability. The remaining two thirds of the organ constitutes a functional reserve. In contrast, when functional subunits are arranged in series (e.g., spinal cord neurons), even a focal injury threatens organ function (e.g., spinal cord myelopathy). Tissues with parallel organization generally have a higher tolerance for radiation than tissues with serial organization. Ablative treatments such as stereotactic ablative radiotherapy are more likely to have an acceptable safety profile when applied in and around tissues with parallel organization or in tissues capable of compensatory hyperplasia after injury than in serially functioning tissues (seen in figure).
Learn more in the Review Article “Effects of Radiotherapy in Normal Tissue” by @DeborahCitrin, MD, and Robert D. Timmerman, MD (@BobTimmermanMD), from the National Cancer Institute and @UTSWMedCenter: nejm.org/doi/full/10.10…
English
Tejaswi Kanala MD retweetledi

I think it is essentially indisputable that future big revolutions in outcome will come from leveraging biology, not technology.
Of course, we should aim to improve the short- and long-term side effects of radiotherapy using technology (there is plenty of room for research in both) and they may interact (such as with lymphopenia-sparing treatments), but ultimately we can't rely on the gizmos to meaningfully bend the curve.
Ralph Weichselbaum@rweichselbaum
@DavidSherMD I also think this whole discussion points out a misdirection of intellectual resources and radiation oncology. I think this infatuation with technology that is relatively minor has diverted the intellectual efforts of the field.
English
Tejaswi Kanala MD retweetledi

To me the TORPEDO (as well as RADCOMP and PARTIQOL) results should cause us to question the assumption that there is a predictable relationship between population-level DVH distribution and individual toxicity profiles. Shifting the *average* DVH to the left (which protons are quite good at doing) did not improve the patient-level experience of side effects. Maybe this is partly due to individual-level variability in dose-response effects, variability that is not captured well by our current approach to DVH-based toxicity analysis, as well as subjective differences in how individual patients experience mucositis and other toxicities.
English
Reading oncology hospice notes is grounding. Patients expressing more regret than gratitude in those moments recalibrate our thinking away from treatment recommendations which implicitly assume longevity alone is paramount.
English
Tejaswi Kanala MD retweetledi

Came to Hyderabad after 41 yrs. Small civil airport at Begumpet was shared with IAF. Now there s sprawling new airport Shamsabad. Cityscape changed. What has not changed is sweet Dakkhni dialect spoken and the sweet nature of people. God bless Hyderabad and its people

English
Tejaswi Kanala MD retweetledi

@TataMemorial Inaugurating the hospital on 28 Feb 1941, the Governor of Bombay Sir Roger Lumley proclaimed: “This hospital is the first large contribution of India to the international fight against cancer.” Sir Sorab Saklatvala called TMH “a labour of love” and “a temple of learning”.
English
Tejaswi Kanala MD retweetledi
Given the heartwarming response to the Foundation Day photo of @TataMemorial, here are some details on the founding of this remarkable institute. Tata Memorial Hospital was inaugurated on 28 February 1941, as Asia’s first comprehensive cancer hospital.
Tata Memorial Centre@TataMemorialCtr
85 years of care, compassion, and commitment. Since 1941, @TataMemorial has remained dedicated to accessible cancer care, advancing research, and training the next generation of oncology professionals. Honouring the legacy. Renewing the commitment. #85YearsOfCare #FoundationDay
English
Tejaswi Kanala MD retweetledi

Study protocol of proton RCT in primary brain tumors (PRIDE) published in @BioMedCentral Radiation Oncology, with study accrual ongoing ahead of schedule @RadOncTMC @ACTREC_TMC @TataMemorial @PTCOG_Official
rdcu.be/e34AG
English
Tejaswi Kanala MD retweetledi

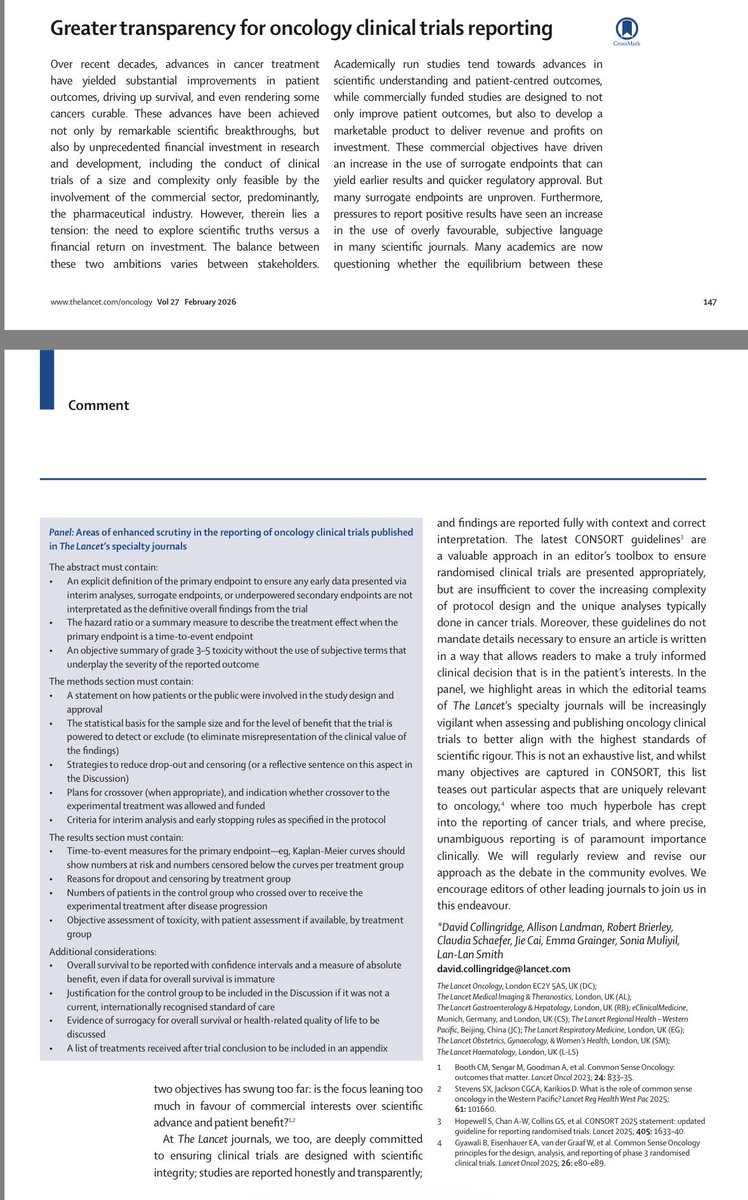
Great to see this important initiative from The Lancet family of journals including @TheLancetOncol highlighting areas of enhanced scrutiny for oncology clinical trials published in the journal, consistent with @csoncol RCT checklist recommendations. It takes courage to lead the change. Very proud of the entire Lancet family of specialty journals for taking this stand. Hoping for a future where “critical appraisal” becomes unnecessary because all trials are reported transparently. thelancet.com/journals/lanon…
English
Tejaswi Kanala MD retweetledi

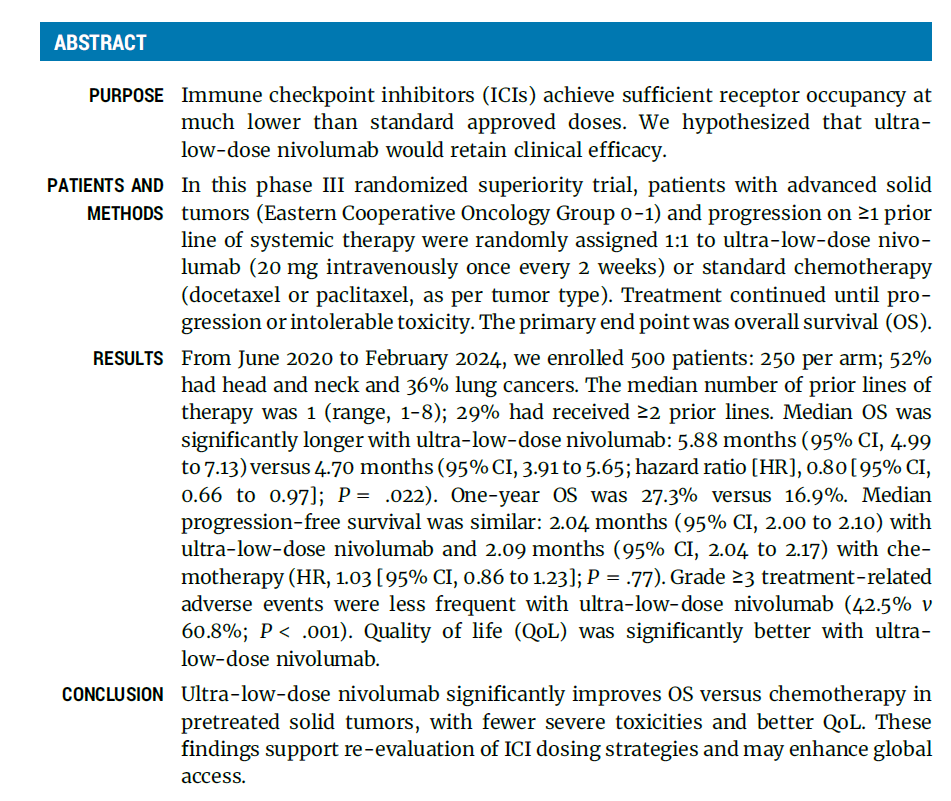
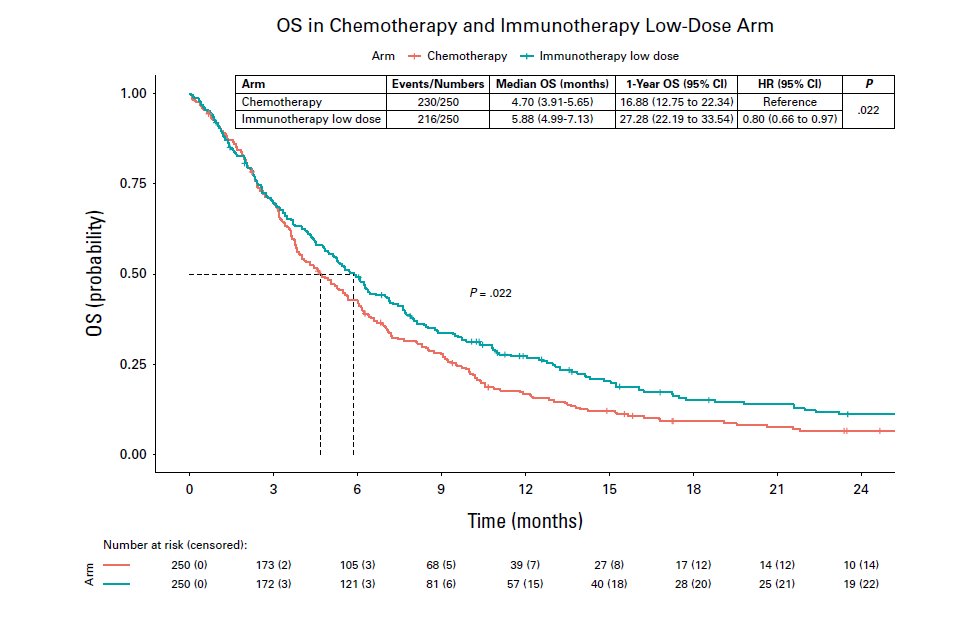
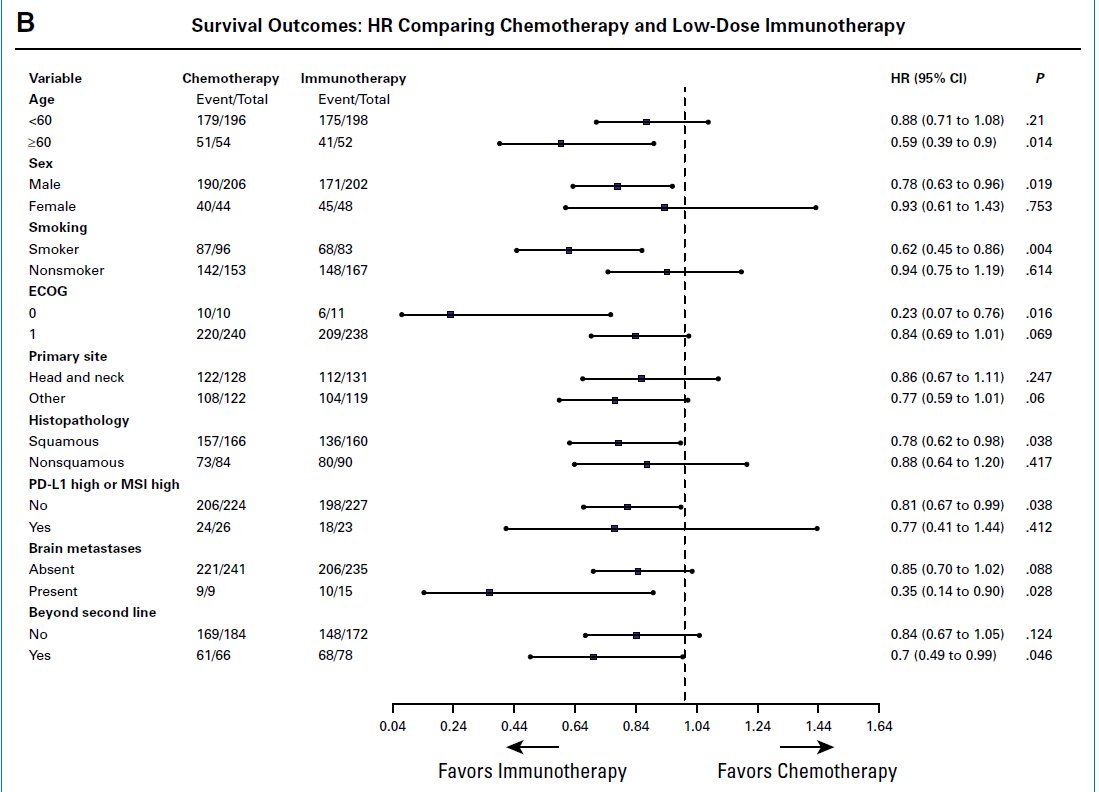
What if we’ve been overdosing immunotherapy all along?
In our Ph III DELII study, 20 mg nivolumab q2w beat chemo in OS, with less toxicity, better QoL. It's time to rethink ICI dosing-for science and equity! ascopubs.org/doi/10.1200/JC… @JCO_ASCO @OncoAlert @TataMemorial @SuyogCancer

English
Tejaswi Kanala MD retweetledi




Tejaswi Kanala MD retweetledi
It’s true because financial toxicity isn’t a sociopolitical issue. It is a clinical issue associated with mortality and poor quality of life, even in public health systems like in Canada. academic.oup.com/jnci/article/1…
Mark Lewis, MD, FASCO@marklewismd
An absolutely damning indictment of the costs of care (in the fiscal meaning of the word): just as many patients fear financial toxicity as death! #GI26
English
Tejaswi Kanala MD retweetledi

Tejaswi Kanala MD retweetledi
A few thoughts on our experience in this oligometastatic endeavor:
- Some patients had a difficult time with randomization to a less aggressive arm. Despite the possibility of salvage SBRT or HN radiotherapy at recurrence, the successful prior history of local consolidative therapy (LCT) made it difficult to accept systemic therapy alone.
- It is challenging to open a cooperative group trial (with little financial benefit) that has a limited patient population. On one hand, only coop trials can answer such a question, but on the other, institutions’ research operations are struggling to stay afloat and are very strategic with what trials they open. We tried to open EA3211 to a wider patient population but didn’t have enough runway to show accrual was feasible with our new criteria.
- In the first-line setting, there are many, many competing systemic therapy trials that pay sites (much) more money per patient and offer the hope of “better" immunotherapy. Especially in this financial environment, it is tough to compete with money.
- However, I also think there is a profound under-appreciation of both the benefit of LCT given its typically modest toxicity and the potential high-grade toxicity of novel systemic therapies. Drugs can cause real harm, and gross disease is the most likely metastatic deposit to recur.
- As we think of new trials in this space, we need to stratify the metastatic population (notice, I did not focus on just OMD) into very distinct cohorts that may benefit from SBRT and other forms of LCT (surgery included). The EORTC formalism is wonderful but complicated (sciencedirect.com/science/articl…), so this approach below (for the sake of discussion on trial concepts) is simplified.
- There are patients with previously untreated de novo disease, who have both primary and metastatic cancer. A critical question is whether we should treat the primary, both to prevent primary progression and its morbidity/mortality and potentially a main source of further metastatic spread. Such treatment can cause acute morbidity but may have the highest yield as a radiotherapy intervention. There are some trials looking at this question, and the benefit likely will profoundly vary by primary site. We included this population in EA3211, but it was too rare to push the trial forward.
- In this same population of previously untreated cancer, managing the metastatic disease is basically a separate question. Here the morbidity of SBRT is much less, and just irradiating each deposit may perform plastic surgery on the scans (saw that language on a previous X discussion) without a long-term clinical benefit, especially since progression is almost always radiographically-detected. I would argue that OS is still the relevant endpoint since salvage SBRT is typically still feasible and efficacious; PFS will make us feel good but not move the needle on more patients living or feeling better. I sincerely hope that we can complete trials in this space, but as we have seen in EA3211, it’s quite tough for the reasons mentioned above.
- In a population that clearly needs systemic treatment, it is absolutely imperative to identify biomarkers (both circulating and radiographic) to distill out patients with detectable (i.e. consider LCT) versus non-detectable disease/MRD. It takes money and collaboration (to generate enough data), but such work (to identify an integral biomarker) is probably the sine qua non of OMD treatment in these patients. The NCI may pay for an integral biomarker in a trial but typically not the research needed to identify one.
- There is a second cohort of patients with previously treated localized disease who now present with new metastases. This group formed the bulk of EA3211 and is probably the most common group of individuals for whom we consider LCT to metastatic disease. To some extent it depends on the time to develop metastases, but here I think we need to focus on a different question than systemic therapy +/- LCT. Patients (and physicians!) may not accept this randomization, competing systemic therapy trials may feel more compelling, and salvage to radiographically-detected progressive mets is feasible (see above). These patients probably need two arms that possess distinctly differently therapeutic approaches.
- Especially in this era of IO (and a few other targeted therapies) that can lead to long-term disease control but with significant toxicities, we should focus more trials on LCT versus systemic therapy (like the HN OMET trial and several efforts in renal cell). Can LCT delay (or prevent) the need to start systemic therapy in a meaningful number of patients? I have had several patients with biopsy-proven metastatic disease cured with LCT, not to mention the group whose systemic treatment was meaningfully delayed. Generally speaking, SBRT is much easier to tolerate than systemic therapy, and this comparison (LCT vs systemic treatment) has many important endpoints, including QoL/PRO and the potential to delay systemic therapy without compromising survival. It will take a change in mindset (mostly among our medical oncology friends) to offer a trial in which patients are not receiving upfront systemic therapy, but personally I feel like this is the way in this cohort.
- There is a final, substantial cohort of patients with growing (or perhaps persistent) metastatic disease despite systemic therapy, where the typical non-LCT approach is second-line therapy. Here is a fantastic opportunity for LCT to show its utility, either from a survival standpoint or by delaying typically less effective and/or more toxic second-line treatment. There is a wonderful recent editorial on relevant, patient-centered endpoints (t.co/TH7FHQhYnd). This oligoprogressive space may be the sweet spot for further trials; the alternative is suboptimal, but the clinical gain needs to be established.
- The forever question of “what is oligometastatic?” is not easy to answer, and the needle is constantly moving and being tested. In EA3211, we used 4 isocenters as the threshold, which was meant to be practical and allow a pretty generous number of metastases (esp in the mediastinum). Personally I believe this is a biological rather than radiologic issue, but we just need to see the results of trials in this space to better understand the possibilities and therapeutic ratios of different SBRT schemes and doses (optimal dose is a whole separate question).
English
Tejaswi Kanala MD retweetledi
It’s out!
It’s very exciting to see the final results of the US phase III RCT of IMPT versus IMRT for oropharyngeal squamous cell carcinoma. Data have been percolating for some time at conferences (and social media), and it’s great to be able to crunch through the actual paper.
I think our community owes a debt of gratitude to the investigators for pulling this trial off. It takes passion, perseverance and just raw time and effort to make such a study happen, and the resultant information is really valuable.
There is a lot to go through here, I’ll start with my final conclusion, which is that IMPT is A, but not THE, standard-of-care for oropharyngeal cancer.
thelancet.com/journals/lance…
English
Tejaswi Kanala MD retweetledi

Ethan Neumann, a 27-year-old PhD candidate in my lab, devoted himself to studying #fibrolamellar carcinoma, the cancer that claimed his life last week.
Please support his father’s effort to establish an endowed research fellowship in Ethan’s name ⬇️
gofundme.com/f/ethan-neuman…

English
Tejaswi Kanala MD retweetledi
I’m also just fascinated/horrified by the increasing traction of inferior local therapies across disease sites. A good amount derives from some longstanding radiophobia that needs to be counteracted but it’s also incumbent on our field and physicians to (proudly) show how far radiotherapy has advanced, in a number of EVIDENCE-BASED ways. Are laterals acceptable for T1 larynx? Yes. But should we settle for them *if* we have other options? I would argue no.
English