Ubaldo La Brocca retweetledi

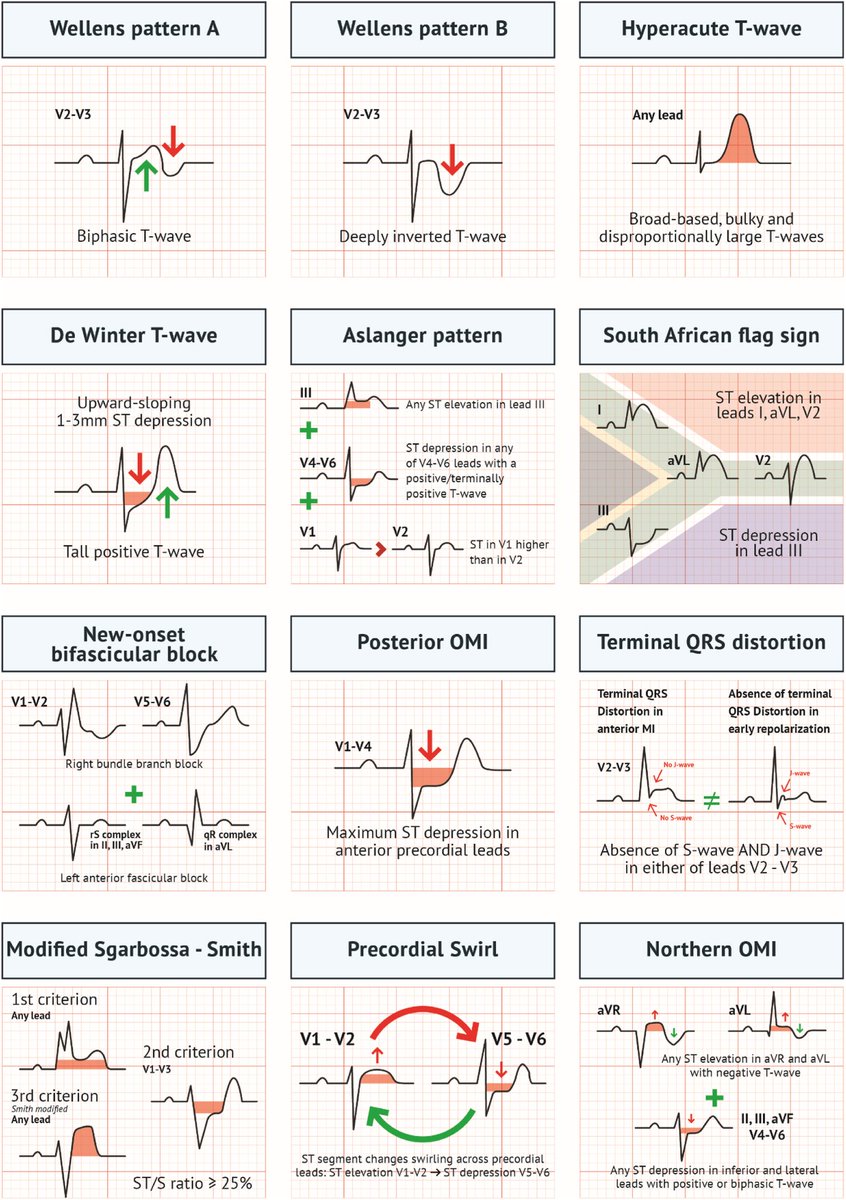
Acute MI is not always STEMI.
A major 2025 review highlights why relying only on classic STEMI criteria can miss dangerous coronary occlusions.
A thread on OMI (Occlusion Myocardial Infarction): 🧵
English
Ubaldo La Brocca
1.6K posts

@baldo_lb
🇪🇺🇮🇹 MD👨⚕️ Pre-Hospital Emergency 🚑 Anesthesia and Intensive Care ⚡️



















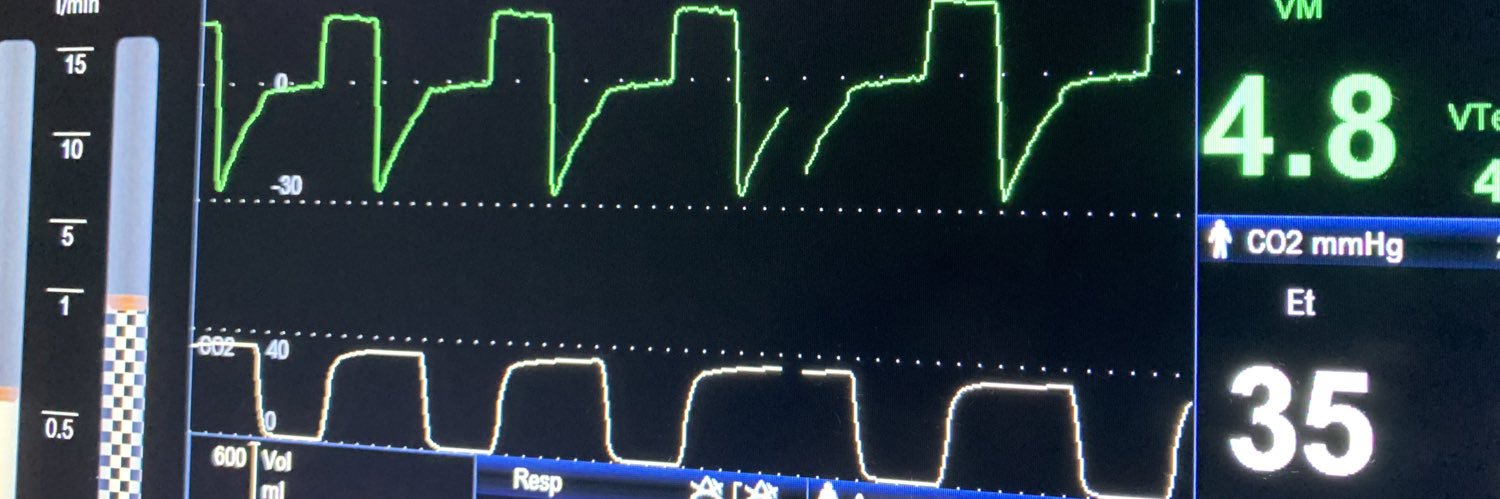
Cardiogenic shock and the DO2 formula The oxygen delivery formula is the only math that matters in a crash! DO2 depends on your Hgb, O2 Sat, and Cardiac Output. Don't be fooled by 100% SpO2—if the pump isn't circulating that "cargo," the organs are still starving.