Benigno Valderrábano Salas retweetledi

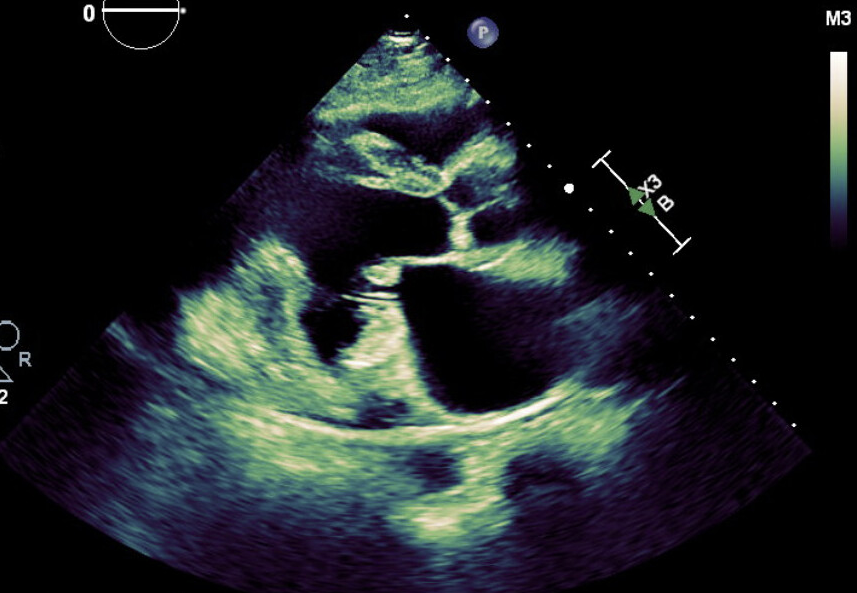
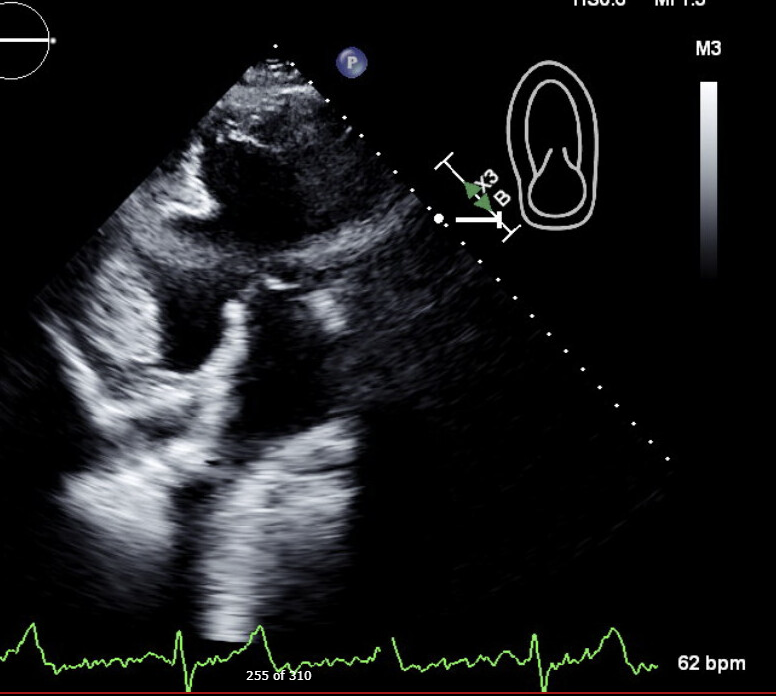
#TR is more than a valve disease. Our review in @ESC_Journals (#EHJHF) proposes a pathophysiology-based framework:
Optimize heart failure, relieve congestion, reassess RV function and comorbidities, then intervene at the right time in the right patient. 🔗doi.org/10.1093/ejhf/x…

English