Sabitlenmiş Tweet

🔑 for those discussing or presenting results at @ASH_hematology! This also applies to us TWEETING about results #ASH25
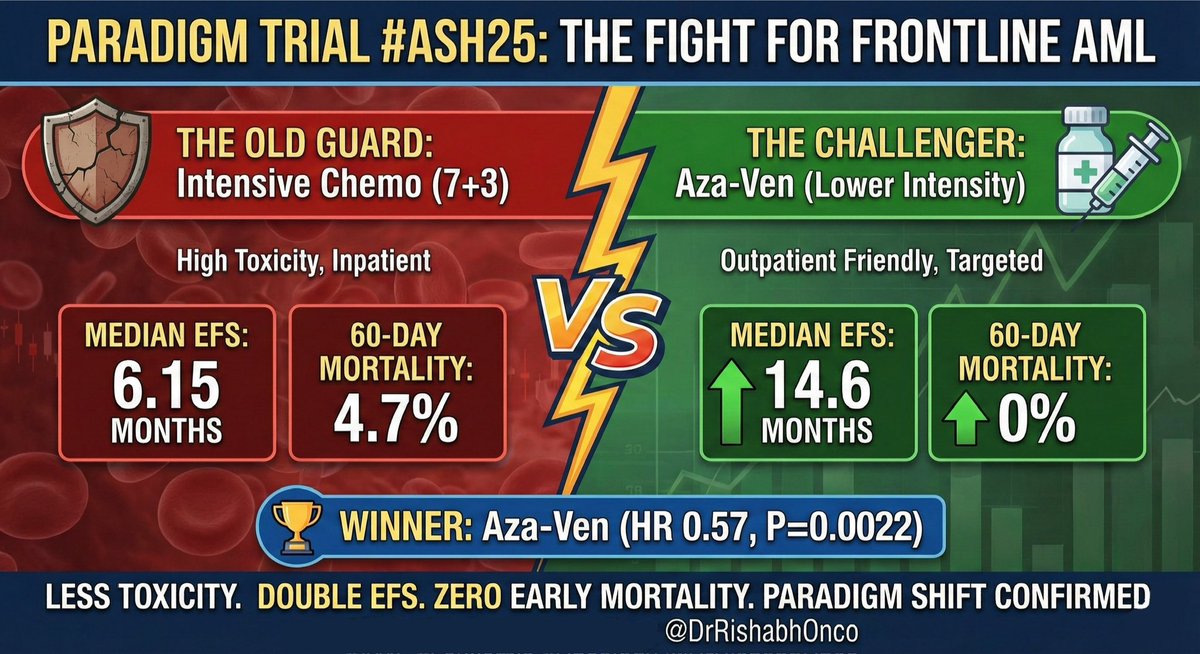
- Present a balanced appraisal - remember, we are caregivers and scientists, not cheerleaders
- do not minimize toxicities or QOL!
sciencedirect.com/science/articl…
English