Salvatore Mattera@SalvMattera
It's been about a year now since I mostly recovered from Long COVID (~90%). Some people said it wouldn't last, but fortunately, it has. No major crashes, no chest pain, no shortness of breath, no nerve pain, no racing heart, no vision issues or any of the other random symptoms that made my life hell for 2-3 years.
What symptoms have remained? My left calf has remained numb to the touch since the 4th COVID infection. My sense of taste has improved but has been muted since the first infection in 2021. My sense of smell comes and goes. I get these bouts of POTS-type symptoms (severe dizziness when standing) that last for a few hours. Not consistently, but typically 3-4 days every month.
What caused me to recover? My hypothesis is that my Long COVID symptoms were/are primarily due to damage to my nerves, which eventually mostly healed. Why mine healed and other people's don't is something someone should be trying to figure out.
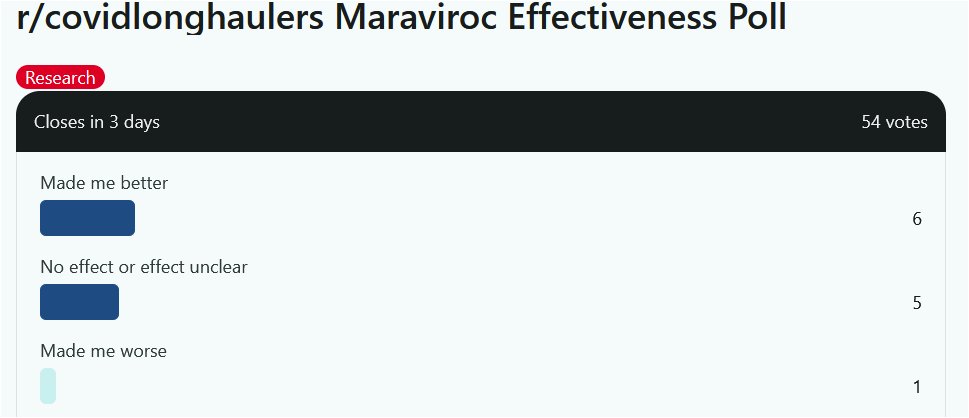
My recovery coincided with my use of maraviroc, lipitor, modafinil, Tirzepatide, BPC-157, LDN, Lexapro, and a bunch of supplements including vitamin D, alpha lipoic acid, etc. I've discontinued all of them, except the Tirzepatide, and have remained recovered. The maraviroc, lipitor, and modafinil were started closest to my recovery (a couple months before), while the others I had been using for many months/years prior. I have no idea if any of these were relevant. Maybe it was just random, and I would have recovered without any of it. Who knows. I got 2 shots of novavax during this time, and am going to get a third soon.
I have remained a committed masker, and have managed to avoid reinfection for about 1.5 years now. Part of this is just luck, because with 2 young kids and a disabled wife, I can't be as COVID cautious as I'd like to be. When she was hospitalized for a month I thought for sure I'd be exposed and catch it, but luckily it just happened to coincide with a time when transmission was low.
At this point, I've accepted that this will probably be as good as it gets, and I've accepted that I'm OK with that. Whereas I used to think of myself as a sick person who was actively dying in a way, I now see myself as a disabled person who isn't in any pain on a day to day basis, but just has some limitations.
I continue to try to advocate mostly because I'm afraid of what happens if/when I get reinfected (maybe nothing, maybe I'll get really sick again?) and also for the many friends I've picked up along the way who remain just as sick as ever. Plus, the prospect of either of my kids getting this is my worst nightmare.