Derek Wu retweetledi

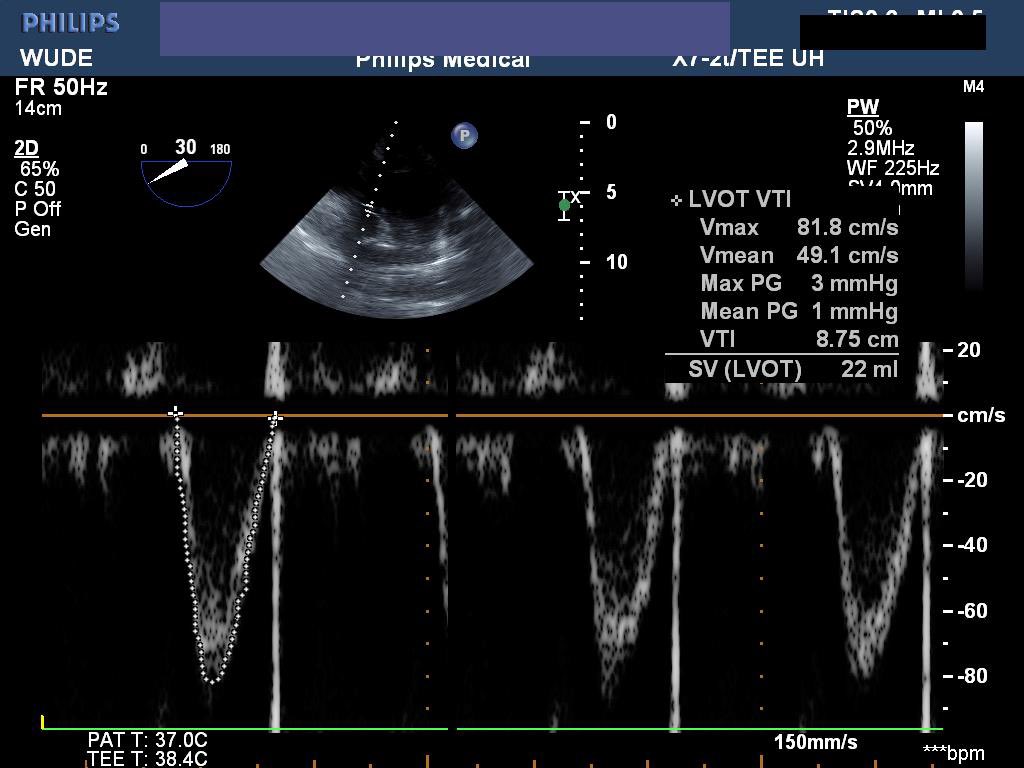
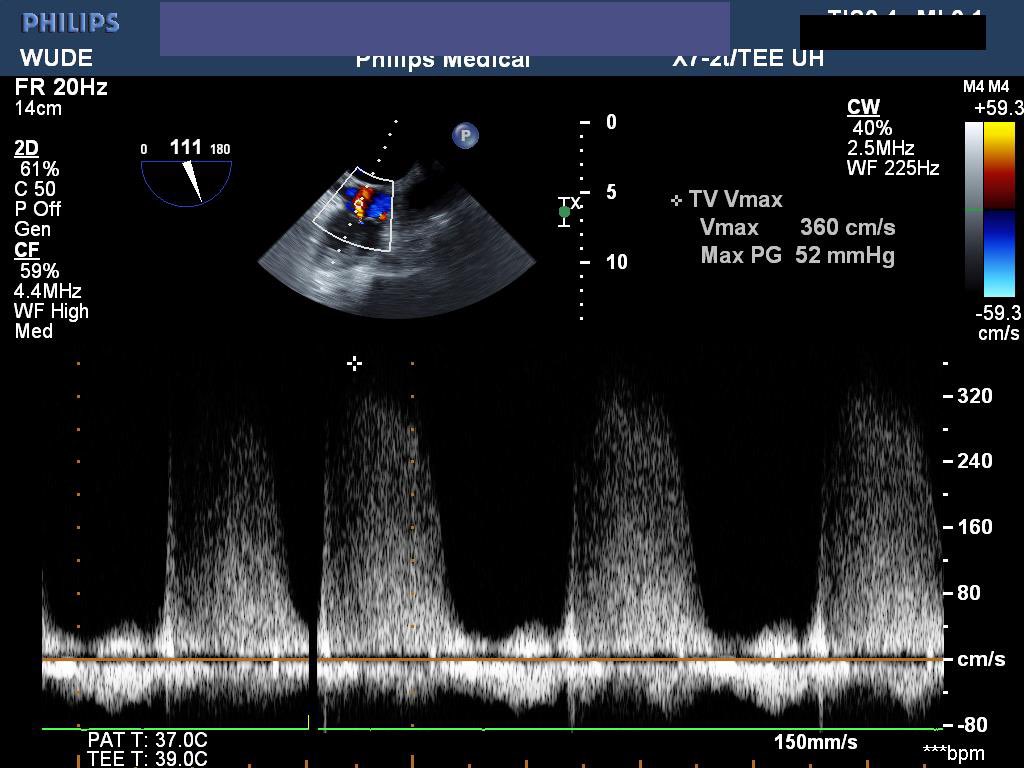
(1/x) Those of us who love #pocus often use it to rule out pneumothorax.
But how reliable is this approach? So-so.
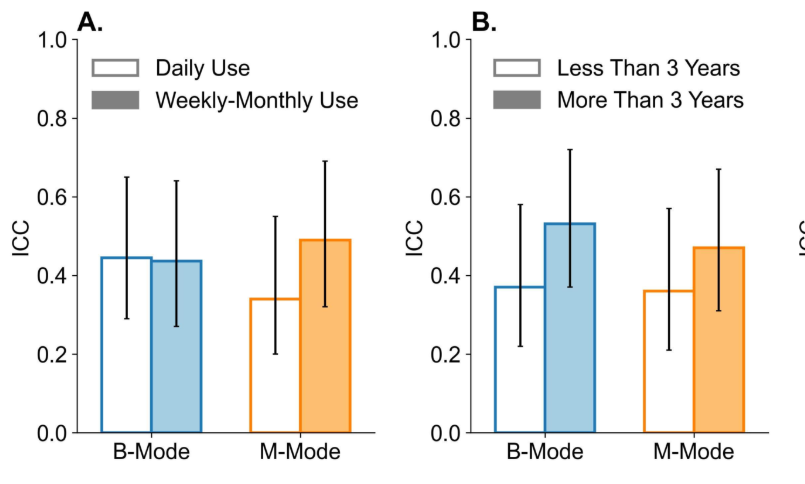
We found only moderate interrater reliability to detect lung sliding among clinicians.
English
Derek Wu
97 posts


@derwuk
@StanfordCCM Fellow | IM @westernuIntMed |#POCUS @westernsono @NBE_96 CCEeXAM Testamur | #deeplearning & #AI @DeepBreatheInc | 🥋🎸🧑💻










As an AI solutions provider in a specialized area of lung ultrasound, it can be a challenge to convey the scale and reach of the problems our team is solving. Our latest video invites you to better understand how we are transforming respiratory imaging! #medtech #ai #ultrasound