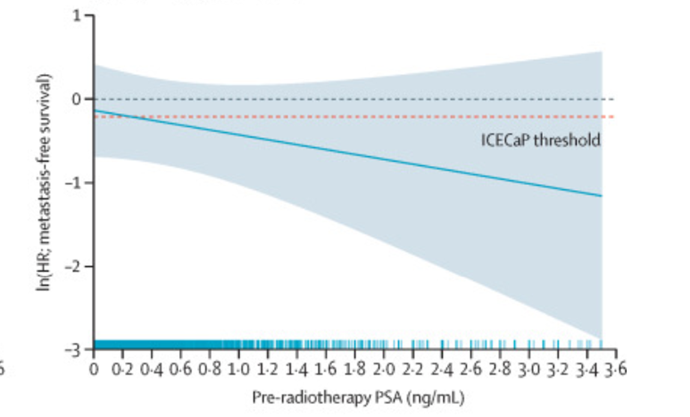
Might this now be possible with the POSEIDON dataset @AmarUKishan?
Calculator showing 10yr MFS with RT (+/- HT) based on pre RT PSA & path features would be v useful, pending widely avail biomarker #radonc #pcsm
Jonathan Tomaszewski@dr_jonathant
Would be really helpful to be able to generate individualised estimates of MFS/PCSS/OS for salvage RT alone (beyond the subgroup data from Supp Table 4). Any plans for a nomogram/calculator, or suggestions re how to go about this? #radonc #pcsm
English