Drue De Angelis retweetledi

I do not believe in accidents.
The system does not need physicians to be wrong.
While physicians argue about vaccines, APPs, RVUs, and IMGs, the architecture dismantling their profession operates without a single opponent in the room.
Section 6001 sits untouched.
CON laws protect incumbent monopolies in 35 states.
Site-neutral payment dies in committee every session.
Professional fees have been cut significantly over the last 20 years.
The Ways and Means contribution tables get filed and forgotten.
Energy and Commerce collected their cash.
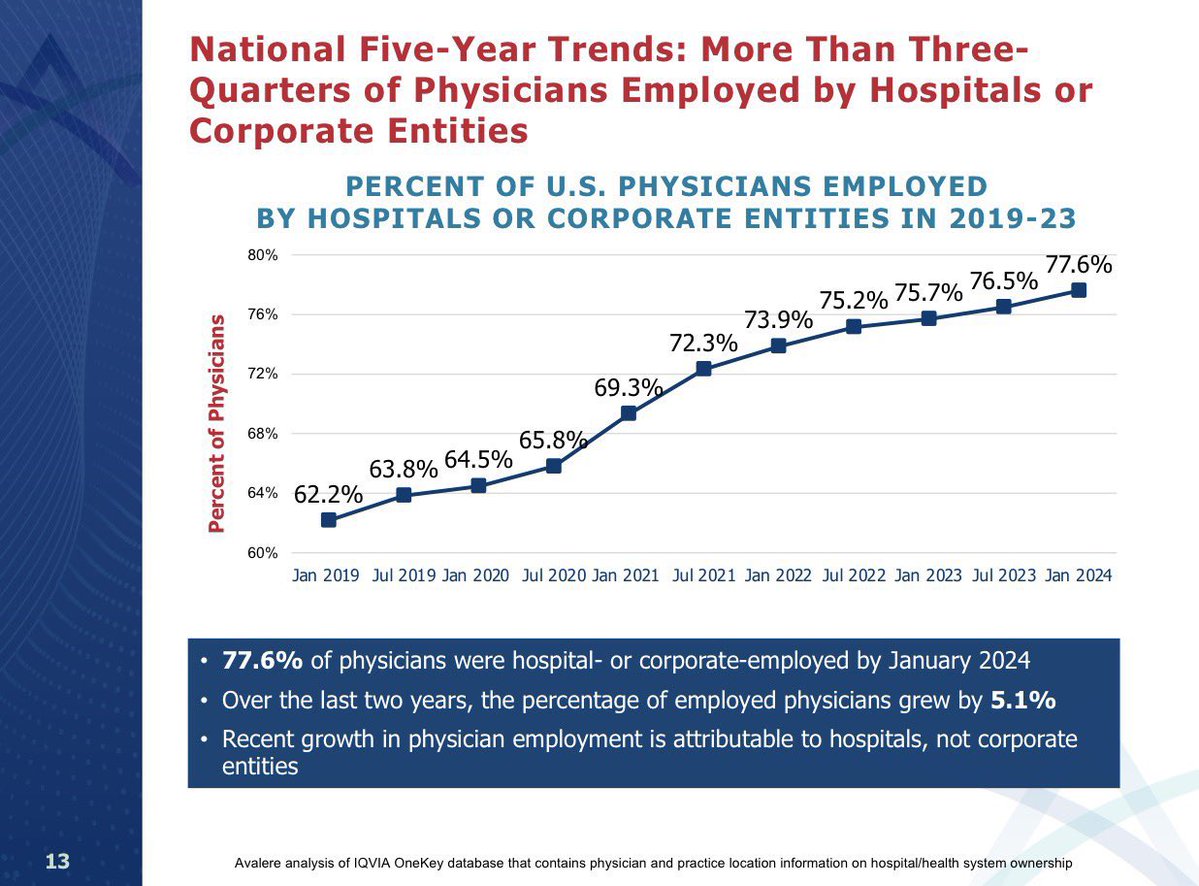
Meanwhile the health system have built a captive architecture around commercial insurance. The employed physicians generate commercial revenue that subsidizes the system.
The system tells the physician they are a cost center. The physician believes it.
The physician does not see the facility fee attached to every service they deliver.
The physician does not see the commercial rate differential between the hospital outpatient department and what they would collect in independent practice.
The physician sees only their salary and the number their administrator shows them.
No hospital ownership and now the lobby is moving to ban ASCs entirely in select markets. Of course this is the last structural alternative to hospital employment for proceduralists who still want independence.
Divided physicians are manageable physicians. United physicians are an existential threat to a $275 billion subsidy apparatus.
Every distraction contains a genuine grievance. That is precisely what makes the distraction effective.
You cannot dismiss a legitimate argument. You can only be consumed by it while the architecture calcifies around you.
The hospital and insurance lobby does not need physicians defeated. It needs them occupied.
As far as I can tell, it’s working…
English