If you're waiting for the frontier models to navigate your EHR and complete physician-level tasks – don't hold your breath.
But, that dawn is just over the horizon.
#FOAMed
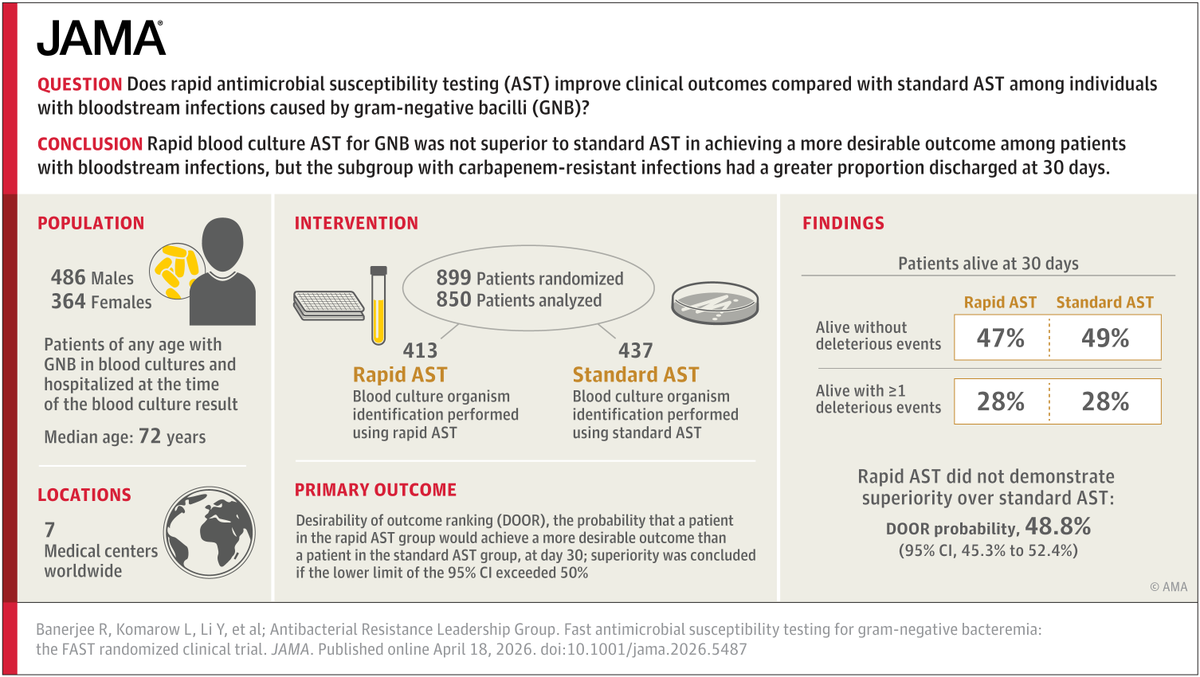
evidencetriage.com/p/can-the-chat…
English
Ryan Radecki, MD MS
23K posts

@emlitofnote
FACEP FACEM AFAIDH. Emergency Medicine & Informatics. @AnnalsofEM Podcast & Journal Club. Columnist @ACEPNow. Speaker, writer, dad. @Stanford '00. 🇺🇸 in 🇳🇿








The feminine urge to type Anthropologie instead of Anthropic


I'll be darned. *That* David Newman is back, and writing about medicine. "Fallen from grace" indeed.