
Greg
4.6K posts

Greg
@gregorythomp
Christian, family medicine physician, OSU and Thunder fan.
Katılım Kasım 2009
471 Takip Edilen280 Takipçiler

I want to sports hate Wemby
He really should be a villain
But I can’t
He’s so easy to root for
I want to see him take down the flopping Thunder so bad
Time to take the throne
English
In residency, I had a patient who established with me with longstanding uncontrolled diabetes, hypertension, and smoking. LDL was average. He came to the hospital with chest pain. We did a CTA, completely clean coronaries. Should we conclude smoking and diabetes don’t matter or that he’s just an outlier?
English

Response to Rebuttals on: "Seven Years of 700 Cholesterol Without Coronary Atherosclerosis".
It’s been really interesting to watch the first 24-hour response to this new paper. The overwhelming majority has been, if not fully enthusiastic, at least curious. And I sincerely appreciate that.
That said, some of the pushback has also been revealing… even comical. So let me address the most common retorts.
⏳1. “He’s too young.”
Asked and answered. HoFH Children with similar LDL and ApoB levels can develop measurable plaque within the first few years of life and even heart attacks by age 8 or 10. Other people around my age, using similar imaging technology, also show measurable plaque. “He’s young” is not a good explanation.
🙄2. “You have a conflict of interest because you’re the patient.”
LMAO! This one might be my favorite. What exactly did I do? Go into the CT scanner and suck in my plaque like I was sucking in my gut? Ask the AI algorithm, “Hey, I’m the patient — do me a solid?” If you think this is a rebuttal, I suggest you don’t join any debate teams.
🦓3. “He’s an outlier.”
Yes. At a population level, I am an outlier. I don’t have obesity, prediabetes, or metabolic syndrome. But that’s one of the broader points: We have a paucity of data on the risks of elevated LDL in metabolically healthy people without underlying genetic lipid disorders.
Outliers are not reasons to stop thinking. They’re opportunities to learn.
🤷♂️4. “It’s a fluke. He’s a one-off.”
What a remarkably uncurious response. Imagine an oncologist had a patient with stage IV pancreatic cancer (~3% five-year survival rate). And that patient somehow cured himself, then went on to win the 100 meters at the Olympics 12 years later.
Would the oncologist say: “Meh… What’s for lunch?”
Of course not. A good scientist or doctor (or curious human) would ask: what happened here?
🧬5. “Oh, you probably just have protective genetics.”
Oh, really? My father had a 99% occlusion of his left anterior descending artery at age 44. My Lp(a) runs between 100 and 194. And on top of that, I have a history of inflammatory bowel disease, a condition associated with chronic systemic inflammation.
🫀6. “But what about the Keto-CTA paper?”
If you’re trying to beat this drum like it’s a trump card, I’d guarantee you’re stuck in an echo chamber and have incomplete information. It has now been clarified repeatedly that the original CLEERLY dataset published on April 7th was not reliable.
CLEERLY had unblinded scans, anomalously results, and refused to perform a quality-control check. And multiple independent analyses have since shown that the KETO-CTA group do not appear to be a high-progression group. This is why we, the authors, took the initiative to retract the paper (NOT the study). The KETO-CTA Heartflow and QAngio data are available as a pre-print. And I’ve seen nobody legitimately try to defend the CLEERLY dataset.
Also, the data show that LDL and ApoB did not predict plaque progression, and even at high LDL and ApoB levels, confirmed regression was observed.
👇
For supporters, feel free to link this the next time you see someone try to deploy these arguments.
For critics, I suggest taking a read and thinking carefully… either to avoid falling onto the pyramid… or to avoid giving me reason to expand it.

Nick Norwitz MD PhD@nicknorwitz
🚨New Paper: "Seven Years of 700 Cholesterol Without Coronary Atherosclerosis: A Lean Mass Hyper-Responder Case Report" Link: doi.org/10.3390/diseas… For the past 7 years, I’ve been running what is essentially a natural experiment in cholesterol and heart health. During that time, I’ve largely lived with: 👉Total cholesterol around 700 mg/dl 👉LDL cholesterol between 500–600 mg/dL I recently underwent advanced coronary CT angiography imaging with AI-guided analysis. This is not a CAC. It measures all plaque (soft + calcified), with expert interpretation and AI-guided analysis capable of quantifying plaque down to the cubic millimeter (mm3). Now, to address the obvious question: Am I too young for plaque? In brief: No. The clearest comparison is individuals with homozygous familial hypercholesterolemia, who often have similarly extreme LDL/ApoB levels and can develop advanced plaque as toddlers, and even heart attacks as early as age 8. Also, nutrition influencers in their 30s have publicly shared quantified plaque scores from these same imaging technologies. In one recent case, a plant-based influencer in his thirties was found to have 61.3 mm³ of plaque despite having far lower lifetime LDL exposure. (He can identify himself if he so chooses.) My case also isn’t a one-off. There are many individuals like me, including older individuals with similar LDL-C and ApoB without any plaque. The difference is that I’m an unusually well-characterized subject, with extensive metabolic data and health markers tracked over time. You can learn more at the newsletter or open-access paper, linked above. The science of heart health is not settled. And cholesterol is not a simple story. 🚨 If you want to help spread the word... Quote Tweet this post (or create an original post) including the article link with a thought. Academic papers are increasingly evaluated using attention metrics. Original posts from unique users are one way to increase these metrics and help ultimately increase its reach. 🚨 If you want to learn more, I'll include more learning resources below 👇
English
@ScottAppliedSci @MurseDarius In residency, I had a patient who established with me with longstanding uncontrolled diabetes, hypertension, and smoking. LDL was ok. He came to the hospital with chest pain. We did a CTA, completely clean coronaries. Therefore, smoking and diabetes don’t matter!
English

@MurseDarius The harsh-sounding answer is, I think, that no one in lipid research is all that surprised. Nothing new, or unexpected, or paradigm-challenging happened. This only surprises people who have a lipid hypothesis straw-man in their minds.
English

#2 is hilarious! 🤣🤣🤣
It baffles me how lipid researchers aren't shoving each other aside to study Nick. Understanding the mechanisms that protect him from heart disease with unprecedented levels of LDL would be incredibly useful in the world of cardiology. But not even just that. I would think self-interest and greed would play a role!!! Imagine being the researcher who identified a new target of therapy or another causal mechanism of atherosclerosis based on studying Nick?
Nick Norwitz MD PhD@nicknorwitz
Response to Rebuttals on: "Seven Years of 700 Cholesterol Without Coronary Atherosclerosis". It’s been really interesting to watch the first 24-hour response to this new paper. The overwhelming majority has been, if not fully enthusiastic, at least curious. And I sincerely appreciate that. That said, some of the pushback has also been revealing… even comical. So let me address the most common retorts. ⏳1. “He’s too young.” Asked and answered. HoFH Children with similar LDL and ApoB levels can develop measurable plaque within the first few years of life and even heart attacks by age 8 or 10. Other people around my age, using similar imaging technology, also show measurable plaque. “He’s young” is not a good explanation. 🙄2. “You have a conflict of interest because you’re the patient.” LMAO! This one might be my favorite. What exactly did I do? Go into the CT scanner and suck in my plaque like I was sucking in my gut? Ask the AI algorithm, “Hey, I’m the patient — do me a solid?” If you think this is a rebuttal, I suggest you don’t join any debate teams. 🦓3. “He’s an outlier.” Yes. At a population level, I am an outlier. I don’t have obesity, prediabetes, or metabolic syndrome. But that’s one of the broader points: We have a paucity of data on the risks of elevated LDL in metabolically healthy people without underlying genetic lipid disorders. Outliers are not reasons to stop thinking. They’re opportunities to learn. 🤷♂️4. “It’s a fluke. He’s a one-off.” What a remarkably uncurious response. Imagine an oncologist had a patient with stage IV pancreatic cancer (~3% five-year survival rate). And that patient somehow cured himself, then went on to win the 100 meters at the Olympics 12 years later. Would the oncologist say: “Meh… What’s for lunch?” Of course not. A good scientist or doctor (or curious human) would ask: what happened here? 🧬5. “Oh, you probably just have protective genetics.” Oh, really? My father had a 99% occlusion of his left anterior descending artery at age 44. My Lp(a) runs between 100 and 194. And on top of that, I have a history of inflammatory bowel disease, a condition associated with chronic systemic inflammation. 🫀6. “But what about the Keto-CTA paper?” If you’re trying to beat this drum like it’s a trump card, I’d guarantee you’re stuck in an echo chamber and have incomplete information. It has now been clarified repeatedly that the original CLEERLY dataset published on April 7th was not reliable. CLEERLY had unblinded scans, anomalously results, and refused to perform a quality-control check. And multiple independent analyses have since shown that the KETO-CTA group do not appear to be a high-progression group. This is why we, the authors, took the initiative to retract the paper (NOT the study). The KETO-CTA Heartflow and QAngio data are available as a pre-print. And I’ve seen nobody legitimately try to defend the CLEERLY dataset. Also, the data show that LDL and ApoB did not predict plaque progression, and even at high LDL and ApoB levels, confirmed regression was observed. 👇 For supporters, feel free to link this the next time you see someone try to deploy these arguments. For critics, I suggest taking a read and thinking carefully… either to avoid falling onto the pyramid… or to avoid giving me reason to expand it.
Carmichael, CA 🇺🇸 English

These referees are absolutely screwing the Lakers. They’re so biased towards Oklahoma City. Tough to watch.
English
@markkaplan20 Actually, deaths from MI are down on a per capita basis at the same time that insulin resistance has skyrocketed. But you already ignored me the last time I said this, so I won’t hold my breath.
English

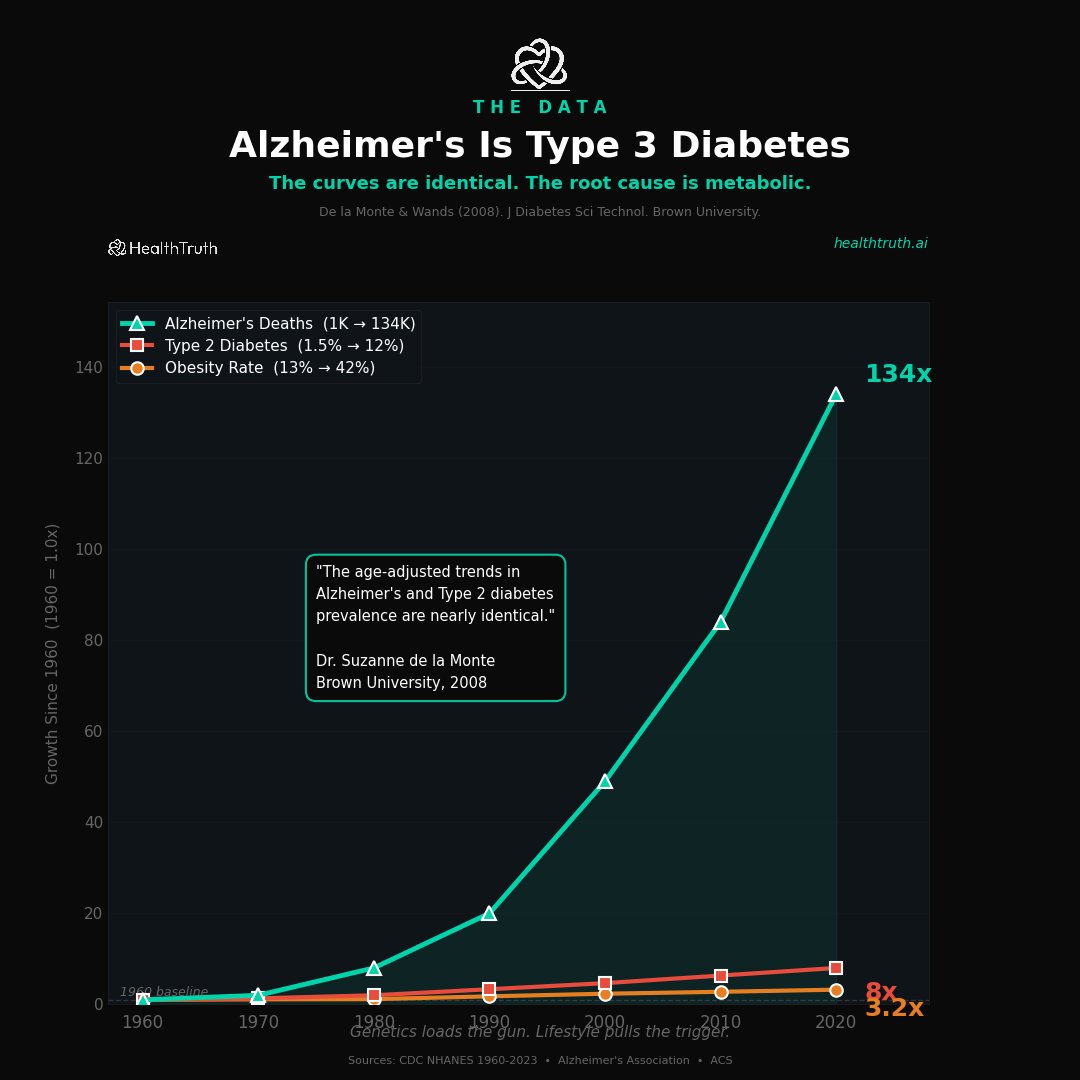
Five diseases. One chart. 50 years.
Obesity up 1,000%.
Diabetes up 637%.
Alzheimer's up 500%.
Cancer up 216%.
Heart disease up 100%.
All rising. All together. All since 1975.
These are not five separate diseases. They are five symptoms of one disease.
A foodborne illness.
The food changed. The guidelines changed. Fat was replaced with sugar. Butter was replaced with seed oils. Real food was replaced with 10,000 chemicals your grandmother would not recognize.
And every one of these lines followed.
Your doctor treats them as five separate problems. Five specialists. Five prescriptions. Nobody connects the dots.
The root cause is metabolic. The science is clear. And the solution starts with what you eat, what you test, and what you stop believing.
healthtruth.ai/neo
The truth heals

English


I don’t know who needs to hear this but deaths from heart disease have fallen >50% since statins were introduced in the 1970s.
This guy = 🦆🦆🦆
Suneel Dhand MD@DrSuneelDhand
I don’t know who needs to hear this, but the mass prescribing of statins has not brought down rates of heart disease In fact, they are higher than they have ever been— and most people being admitted to hospital with heart issues are already on statins Ask more questions, folks!
English
You are correct. Better treatments in other domains are the reason for an increase in Alzheimer’s deaths. But—and I’m glad you agree— age adjusted Alzheimer’s diagnoses are down at the same time insulin resistance and diabetes has sky rocketed.
Also, interestingly, age adjusted deaths from cardiovascular disease have plummeted too, at the same time insulin resistance has sky rocketed. I’m sure you’ll point to better MI care and less smoking, which is correct, but LLT plays a role in that too. It all does. Smoking, blood pressure, lipids, glucose. (I’d actually argue BP is underrated and gets no attention on social media, but alas). All risk factors matter. And for you to discount life saving drugs for many, is a real shame and quite odd.
You say your doctor only focused on lipids after your MI. Well, they suck as a doctor. Level 1, basic, medical school training is to look at blood pressure, smoking, diabetes, lipids, and obesity/diet/exercise.
English
Good chart. And the data is real. Age-specific incidence has declined at each age group.
But total Alzheimer’s deaths have still exploded from 1,000 to 134,000. Both things are true at the same time.
The decline in age-specific rates likely reflects better cardiovascular care keeping people alive longer. Blood pressure drugs. Surgical interventions. We got better at stopping people from dying of heart attacks. So more people survive into the age window where Alzheimer’s develops.
That is not a victory. That is keeping people alive longer while the metabolic environment that causes neurodegeneration gets worse.
The question is still the same. What is driving the metabolic dysfunction. And can we prevent it before the brain is damaged.
English
My Alzheimer's thread hit 604,000 views this weekend. Bill Ackman shared it. Doctors debated it. People sent it to their cardiologists.
But a lot of people asked me the same question. Show me the data.
Here it is.
Alzheimer's deaths, Type 2 Diabetes, and obesity. All indexed to 1960.
Alzheimer's deaths have exploded 134x.
Type 2 Diabetes. 8x.
Obesity. 3.2x.
Same timeline. Same inflection point. Same curve.
This is not genetics. Genetics do not change in 60 years. This is a man-made disease. The chart is the proof.
English
@markkaplan20 You’re quoting a women’s study as a man. The hazard ratios are different for men. As a heart attack survivor, you’re declining a medication that’s shown a reduction in all cause mortality by 30% at 5 years. Good luck 🤷🏻♂️
English
So if cholesterol is not the main driver, what is?
The Womens Health Study followed 27,939 women for 21 years. Published in JAMA Cardiology.
They measured every risk factor and ranked them by how much each one actually predicted heart disease.
LDL cholesterol was 1.4x. Total cholesterol was 1.0x. Barely moved the needle.
Diabetes was 10.0x. Metabolic syndrome was 6.0x. Severe obesity was 4.7x. Hypertension was 4.0x. Smoking was 4.0x.
The green bars on this chart are what your doctor focuses on. The red bars are what actually kills you.
My doctor tested the green bars 11 times in 12 years. He tested the red bars zero times.

English
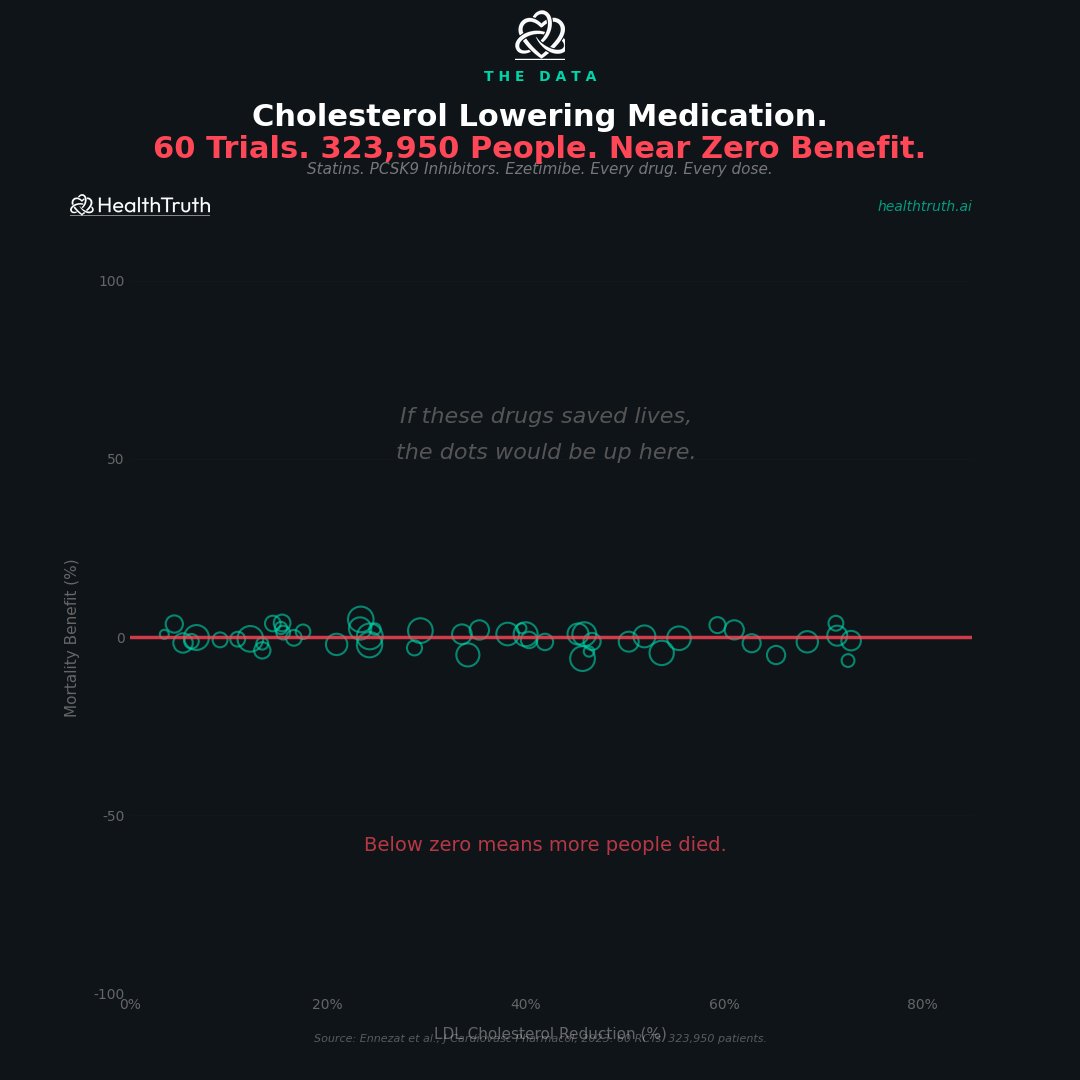
My doctor put me on a statin after my heart attack at 52.
I trusted him. I took the pill. I never asked a question.
Then I found this study. 60 clinical trials. 323,950 people. Every cholesterol lowering drug ever made. Statins. PCSK9 inhibitors. Ezetimibe.
They measured how much each drug lowered LDL cholesterol. Then they measured whether people lived or died.
The line is flat.
It did not matter if they lowered LDL by 10% or by 70%. The death rate did not change. In some trials people died more.
323,950 people. Near zero benefit. Published in the Journal of Cardiovascular Pharmacology. 2023.
Nobody showed me this chart. Not my cardiologist. Not my pharmacist. Not the drug rep who visited my doctors office every month.
I had to find it myself. After the heart attack.
English
@HPbasketball @MikyBerra Sports brings out our most primal and irrational instincts. Until someone watches every foul and breaks it down, I say we stick with the numbers.
English
@MikyBerra Number specific isn’t the best way either. You’d need to go back and watch every foul drawn to assess it from multiple angles and every defensive possession the same. I’ve said there is no data evidence. But also you only take this position BECAUSE it benefits you
English

Evaluating officials when Okc is involved is surely interesting, not trivial, but interesting.
But the way Matt poses it is a classic “thinking fast & slow” issue.
Discussing quantitative stuff with perception “feels like something is off” instead of “statistically…” 1/
Hardwood Paroxysm@HPbasketball
Thoughts on officiating: - Fans always feel their team gets screwed, but universally, everyone watching OKC feels like something is off in how they're officiated. That matters. It just does. OKC Fans will claim jealousy or hate because the alternative is untenable for them. But there is a genuine feeling among all fans that the disparity in SGA's whistle to their defensive whistle is incongruous - The next step is the "So you think the league is rigging for a small market team?" and I understand the consequential thinking, but I think it's healthier to just focus on the problem. I think there's no grand conspiracy but there IS an incongruity in officiating. - Last year, we had an awesome first round, in which the players were openly pleading to be less physical because they felt it was dangerous. So now we've gotten a regular-season whistle. And it sucks. As fans, we hate it. I don't know what that balance should be because it's not my body on the line, but it sure feels like there's a way to have a physical contact sport set of officiating perameters that also deters dangerous play - Finch was campaigning to try and politic a win, but he also wasn't wrong when before Game 2 he made the point that the call should be based on what happens at point of contact and not what happens afterward (flop/flail/fall). The contact is what needs to matter and not the sell job after it. - Shai is genuinely difficult to officiate because he IS incredible at driving and controlling where he goes to challenge direct path defense. It's a genuine skill he has. - He also sells because otherwise he doesn't get the call. This is maybe the biggest problem of all: if you legitimately create the contact but don't performatively exagerate it, you will not be rewarded. That's a problem. - We always find something to say is a problem with the NBA, and more so in the playoffs when it's in the spotlight. But this is a genuijne issue for watchability. Fans don't want this. The league needs to listen.
English
@TheSecondCutPod @RickRunGood @therealGFD @mark_immelman Piggybacking on Mark’s spitballing: Rolapp should make a special 72 hole event with former LIV players and the winner gets back on the PGA tour immediately.
English



@DrJesseMorse @ScottAppliedSci Jesse, why has cardiovascular disease death fallen dramatically at the same time insulin resistance has risen substantially?
English

Andrew, please explain something to me
You guys have been focused on LDL for the past 30 years
Every year you continue to lower the target range
Yet just like 30 years ago, cardiovascular disease is still the number one killer in the United States
Obviously statins aren’t the answer
Time to start looking in other places, namely, metabolic syndrome, insulin resistance, blood pressure, etc
English
The anti-statin folks have mostly lost their minds and fully lost their integrity.
He compares absolute risk reduction for statins with relative risk reduction for the Mediterranean diet - while claiming "head-to-head" comparisson.
And, the usual suspects uncritically retweet.
Mark Kaplan@markkaplan20
🧵 Statins vs Mediterranean Diet. Head-to-head. Same outcome. Let the studies speak. STATINS (primary prevention): → Absolute risk reduction: ~1% → NNT: 200+ people treated to prevent 1 event → Side effects in 20%+ of patients → $15 billion annual market (Taylor et al., Cochrane, 2013) MEDITERRANEAN DIET: → ~30% reduction in cardiovascular events → No side effects → Costs: olive oil, nuts, vegetables, fish → Market value: $0 (can't patent food)
English

@DrJesseMorse @MichaelAlbertMD And heart disease death on a per capita basis has plummeted. Makes you think!
English
@MichaelAlbertMD You guys have been targeting LDL for 40 years yet heart disease is still the #1 killer in the US
Maybe it’s not LDL?!
English

I'm tired of watching people die from preventable heart disease.
The cholesterol wars are over. LDL causes atherosclerosis. That's not a pharmaceutical talking point—it's the convergent conclusion of genetics, Mendelian randomization, and 170,000+ patients across 26 randomized trials.
Next week, we put diet tribalism and LDL denialism aside and go straight to the science that saves lives.
Sign up to receive my newsletter: substance-over-noise.beehiiv.com

English
@NewLeafs2016 @MichaelAlbertMD Then why has heart disease death gone down at the same time consumption of those has gone up?
English

@MichaelAlbertMD Atherosclerosis is caused by seed oils, processed sugars, and much of the modern 'diet', which consists of highly refined products that should not even be classified as food.
LDL has zero to do with it.


English

@ethanjweiss @radfugee Amazing this is essentially the opposite of what the keto zealots want. Bizarro world.
English
Another win for the lower is better crowd…
Intensive LDL Cholesterol Targeting in Atherosclerotic Cardiovascular Disease | New England Journal of Medicine nejm.org/doi/full/10.10…
English
@DrNadolsky …combinations of carbs and fat are the most addictive. Good times.
English
@DrNadolsky One time, he posted that carbs are the most addictive food linked a paper. I said that’s ridiculous and that combinations of carbs and fat are the most addictive. He then got all pompous and said why don’t you teach me. So I screenshotted the paper he linked that said…
English

When you have an 'I hate my job' day, try this out:
Stop at your pharmacy, go to the thermometer section & purchase a rectal thermometer made by Johnson & Johnson.
Be very sure you get this brand.
When you get home, lock your doors, draw the curtains and disconnect the phone so you will not be disturbed.
Change into comfortable clothing and sit in your favorite chair. Open the package and then remove the thermometer and place it on a flat surface so that it will not become chipped or broken.
Now the fun part begins.
Take out the literature from the box and read it carefully. You will notice that in small print there is a statement:
"Every rectal thermometer made by Johnson & Johnson is personally tested and then sanitized."
Now, close your eyes and repeat out loud five times, "I am so glad I do not work in the thermometer quality control department at Johnson & Johnson."
English