Maria F Teixeira retweetledi

1/n
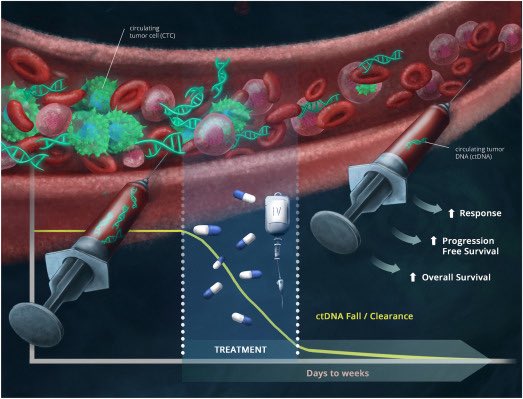
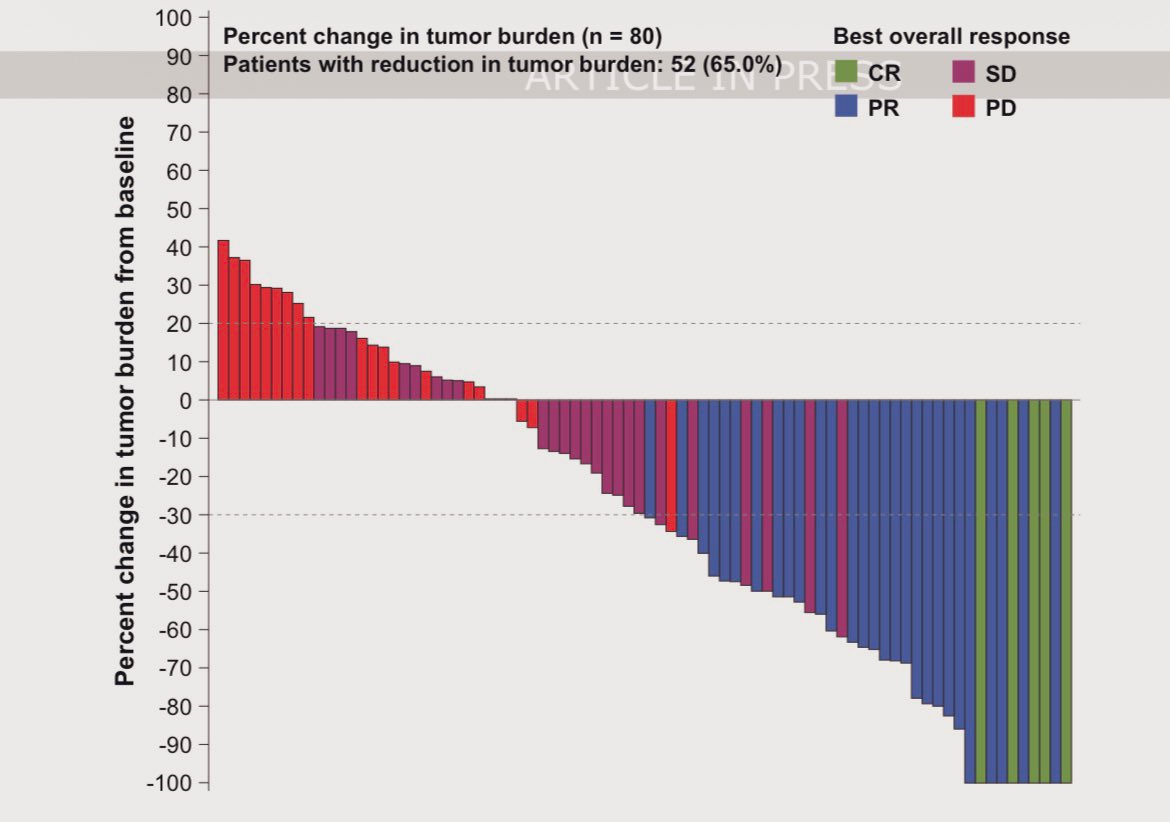
Daraxonrasib (RMC-6236), the first-in-human oral 💊RAS(ON) multi-selective tri-complex inhibitor, in previously treated RAS-mutated pancreatic cancer phase I/II study is now published in the New England Journal of Medicine @NEJM
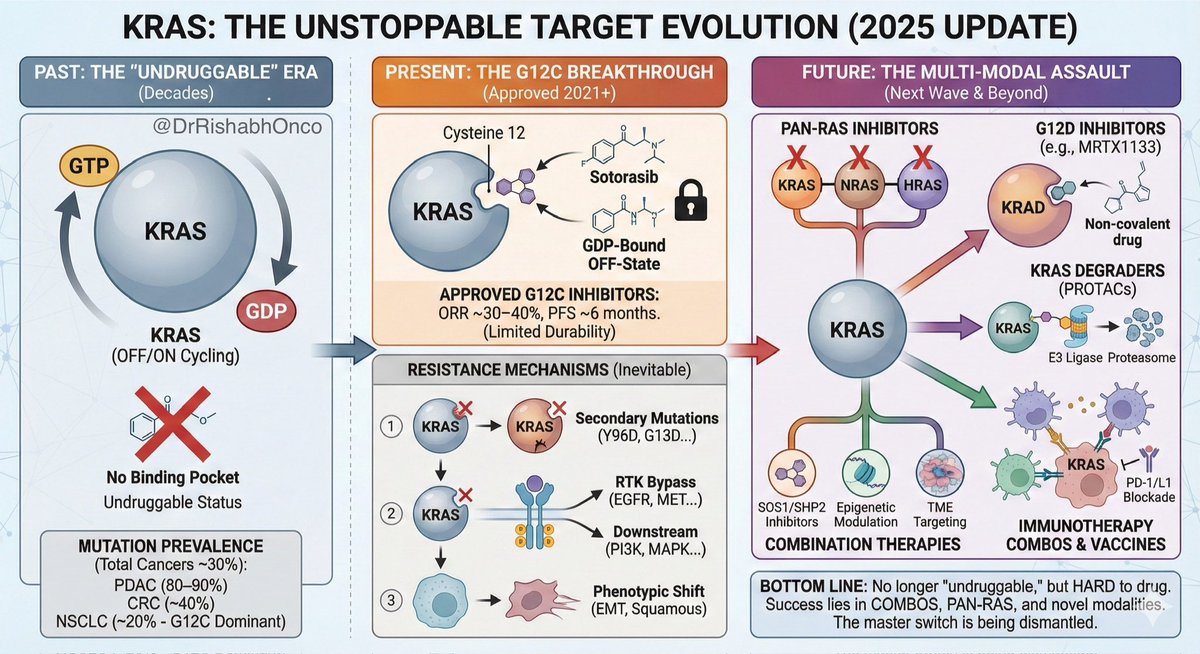
A novel💡 way to shut down ⚔️RAS, one of the most important oncogenic drivers in cancer that had long been considered “undruggable.”
🔗nejm.org/doi/full/10.10…
Shout out to Brian Wolpin, @CentralParkWMD @GarridoLagunaMD @AlexSpiraMDPhD @salmanpunekar @MeredithPelster @bherzbergmd Nilo Azad Aparna Hegde @DavidHongMD and the whole team who dedicated to this study. @EileenMOReilly
#HBP #HumansBeyondPatients
Manhattan, NY 🇺🇸 English