Mark Fahlen retweetledi

Now open access in @NDTsocial
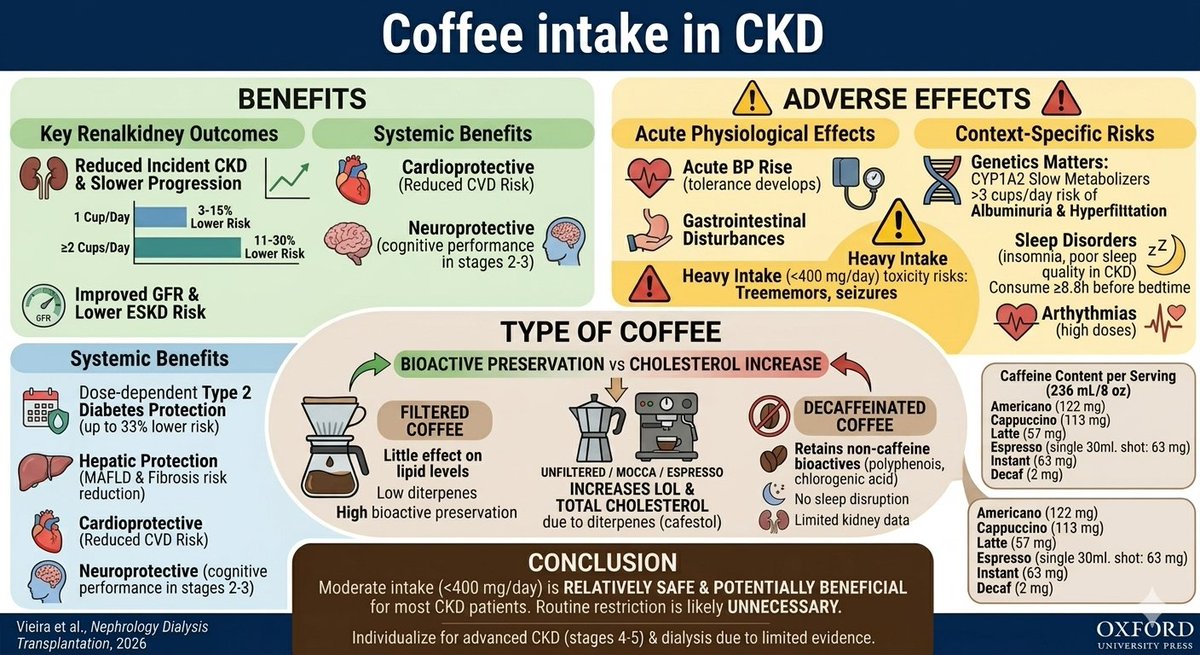
Coffee consumption and chronic kidney disease
🧐Current evidence suggests that moderate caffeine intake is probably safe in CKD and may be potentially beneficial.
▶️academic.oup.com/ndt/article-ab…
English