Meredith Olsen, MD retweetledi

One of my favorite aviation phrases:
“Superior pilots use their superior judgement to avoid having to demonstrate their superior skills.”
It’s true for any proceduralist btw.
English
Meredith Olsen, MD
41 posts


@MereLOlsen
CCM. Love the RV, a good shock exit strategy and MedEd.
I just read this outstanding review by Prof. Michael Pinsky: 👉 “The Effective Management of Shock: From Physiology to Guidelines to Personalized Medicine” 🧠 Key paradigm shift: 👉 Shock is not about numbers 👉 It is about tissue perfusion and cellular metabolism ⚠️ Three brutal truths (often ignored in daily practice): 1️⃣ Once organ injury occurs → we cannot reverse it → We can only limit further damage 2️⃣ Monitoring alone does not improve outcomes → Only actions linked to effective therapies matter 3️⃣ Guidelines ≠ patient care → The clinician’s physiologic reasoning remains central 📊 Why many “standard” approaches failed: Targeting DO₂ “supranormal” levels → ↑ mortality EGDT bundles → not superior to good early care Fixed 30 mL/kg fluids → harmful in non-responders 👉 Lesson: One-size-fits-all resuscitation is physiologically wrong 🫀 Modern hemodynamic thinking: ✔️ Fluid responsiveness matters (PPV, SVV, PLR) ✔️ MAP alone is not enough ✔️ Focus on: Tissue perfusion pressure Critical closing pressure (Pcc) “Vascular waterfall” concept 👉 Increasing MAP ≠ improving microcirculation 🔥 Game-changing concept: 👉 Shock = failure of microcirculatory flow regulation Even with: Normal CO Normal MAP ➡️ Tissue hypoxia may persist 🧬 The real goal of resuscitation: ❌ Normalize numbers ✅ Restore effective tissue perfusion early ✅ Avoid iatrogenic harm 💡 Where we are going: Capillary refill time (CRT)-guided resuscitation Personalized MAP targets Dynamic physiology-based decisions AI-driven precision resuscitation 📌 Take-home message: 👉 The future of shock management is NOT: More fluids More drugs More devices 👉 It is: Better understanding of physiology + individualized care 🧠 And maybe the most important sentence in the paper: 👉 “The thoughtful bedside clinician remains the gold standard.” #CriticalCare #Shock #Hemodynamics #ICU #Sepsis #PersonalizedMedicine #Resuscitation #Pinsky

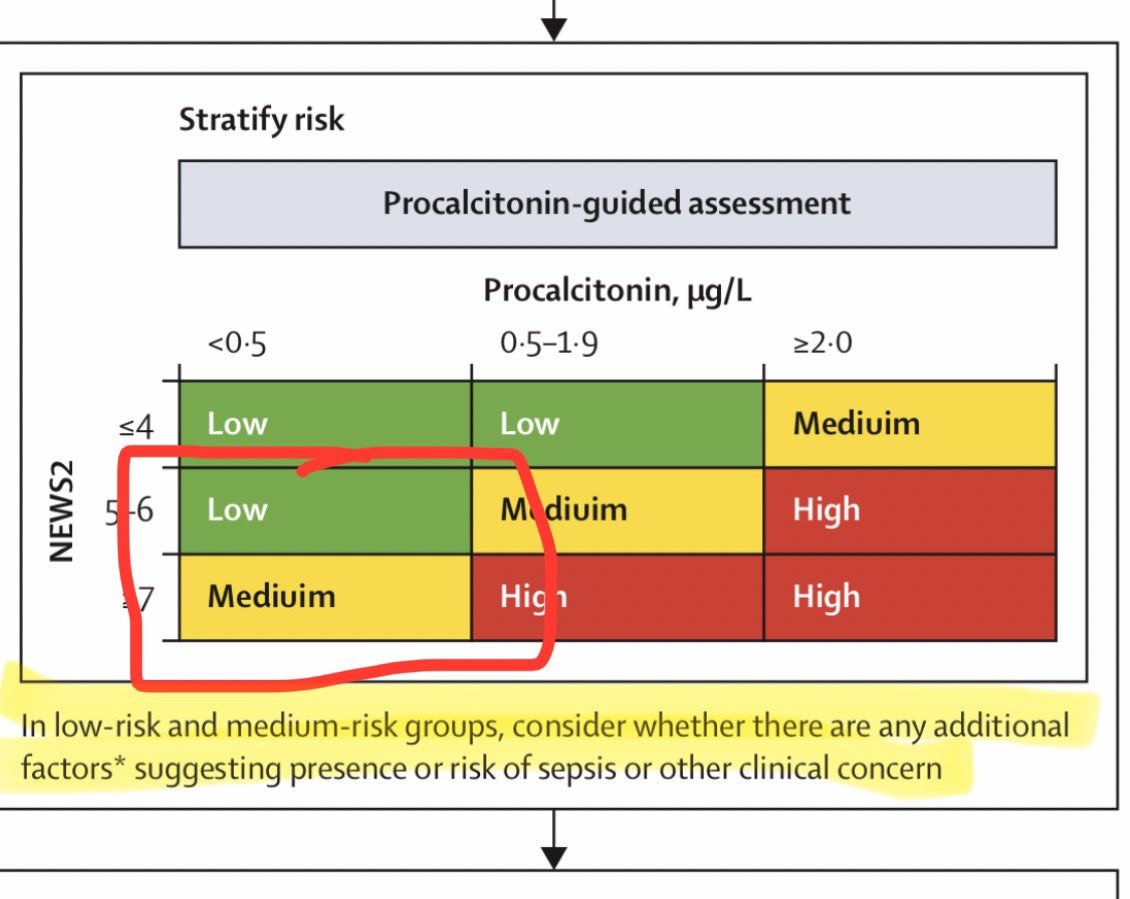
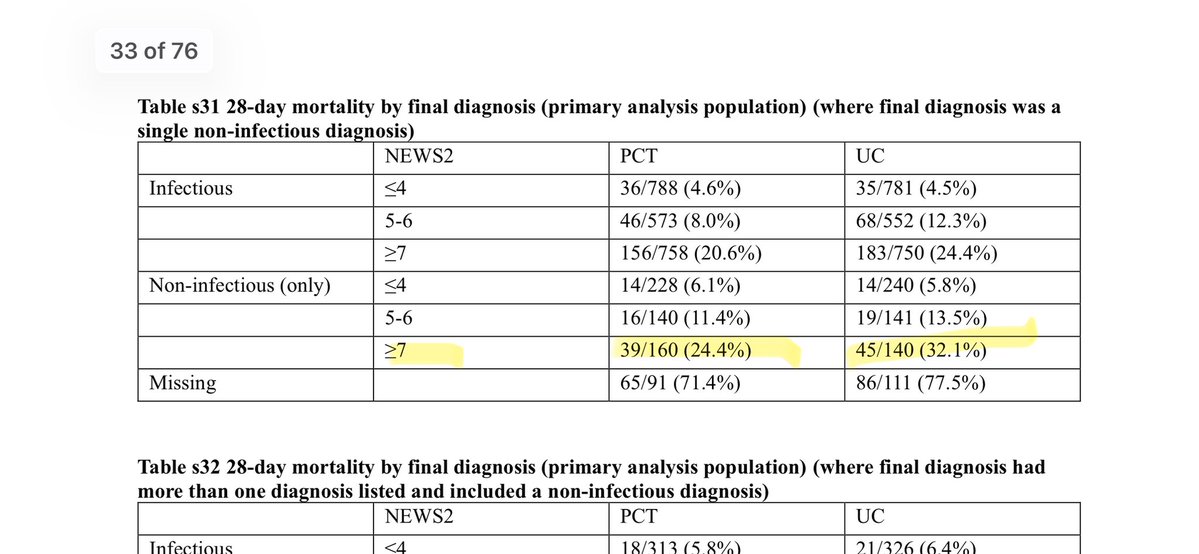
The results of the PRONTO RCT of procalcitonin in people with suspected sepsis are absolutely fascinating. Mortality was significantly lower in the procalcitonin-guided care group: 13.6% (372/2738) vs 16.6% (450/2715) (p=0.0009) but there was no difference in antibiotic initiation, narrowing, or days of therapy! So apparently procalcitonin saves lives even if it doesn’t change antibiotic prescribing? 🤔 1/












Paracetamol significantly reduced cerebral temperature in febrile brain-injured pts (overall mean reduction of 0.6°C), maintaining temperatures <38.5°C for a median of 3.6 hours. 🧠 shorturl.at/sK5Eq #SCCMNeuro #NeuroICU #NeuroTwitter #NeuroX
