Sabitlenmiş Tweet

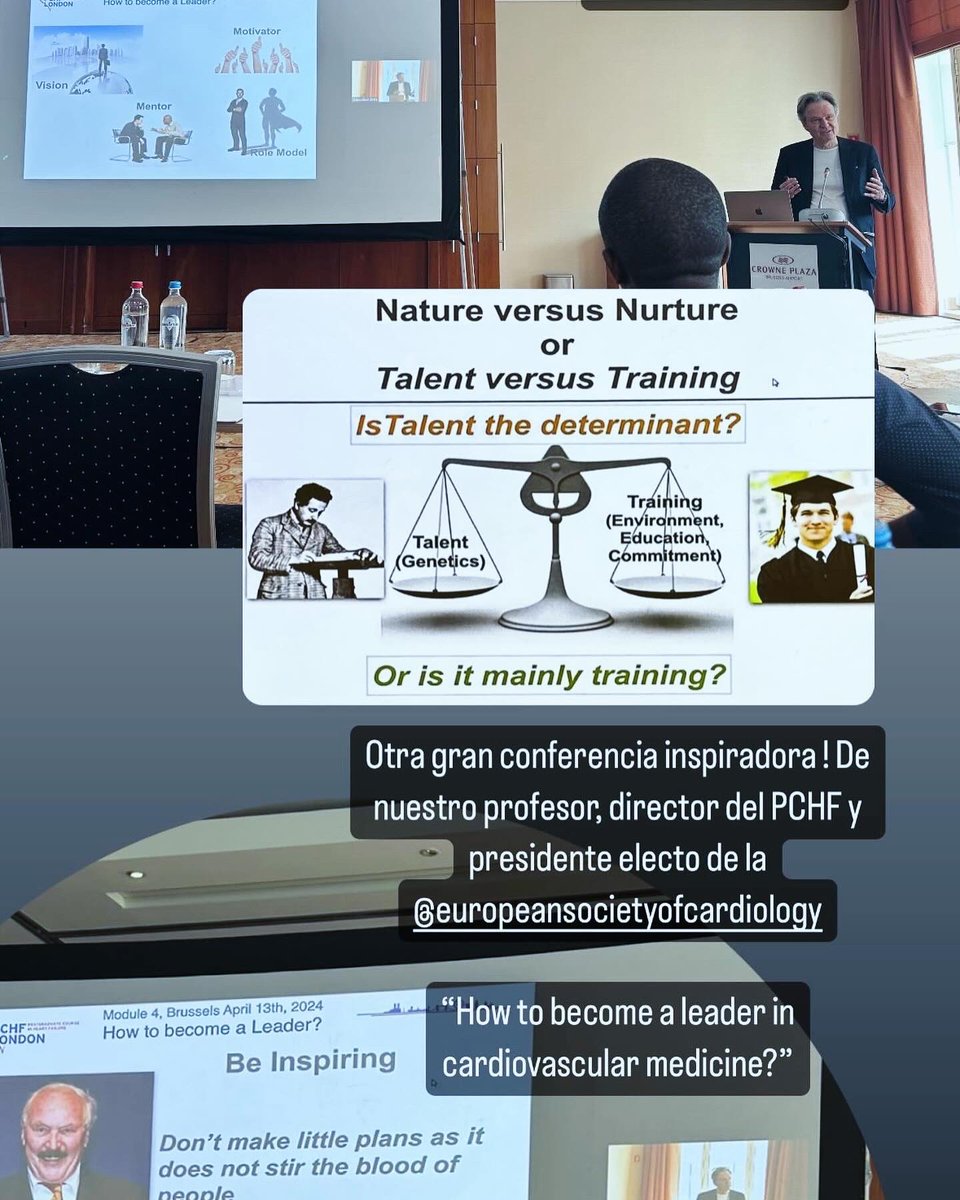
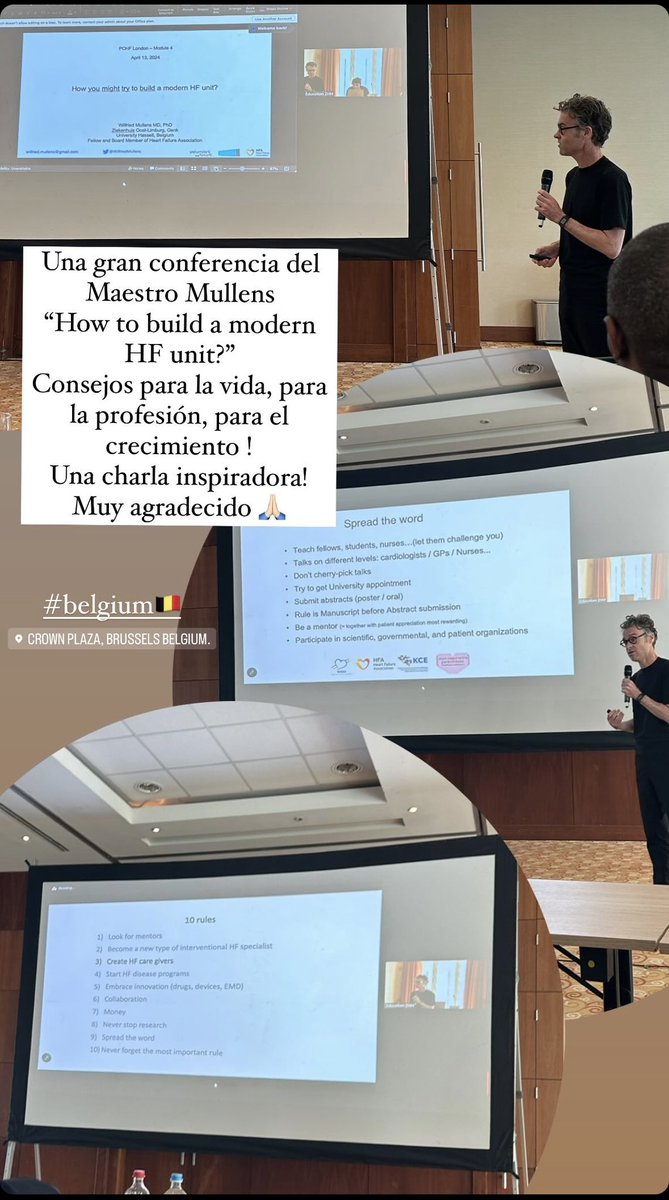
Heart failure days and Belgium 🇧🇪 experiences 🫀!
“If I have seen further, it is only by standing on the shoulders of giants” Newton. @WilfriedMullens @TomLuscher @ehj_ed @zhh_ch
#PCHF #Heartfailure #insuficienciacardiaca #cardiology #academy #brussels #belgium


La Calera, Colombia 🇨🇴 English