
stefano parlamento
906 posts

stefano parlamento retweetledi

A new JAMA piece by serious statisticians warns that Bayesian methods threaten “objectivity” and “replicability” in confirmatory trials. These aren’t cranks — Fleming and Evans have forgotten more about clinical trials than most of us know. And they’re still wrong. Here’s why. 🧵
English
stefano parlamento retweetledi

MAP doesn’t determine mean systemic pressure.
MAP doesn’t cause flow.
This is basic haemodynamics / physics.
If we get the fundamentals wrong in guidelines, it's no wonder clinicians get confused.
Philippe Rola@ThinkingCC
Wait what??? MAP a driver of VR and CO??? SSG26 is any physiologist reviewing this? @icmteaching what do you think? @EMNerd_ flagged this quick! @khaycock2 @PulmCrit @emcrit thoughts? all MAP not created equal, and that most msfp is venous. MAP does not drive VR. Come on…
English
stefano parlamento retweetledi
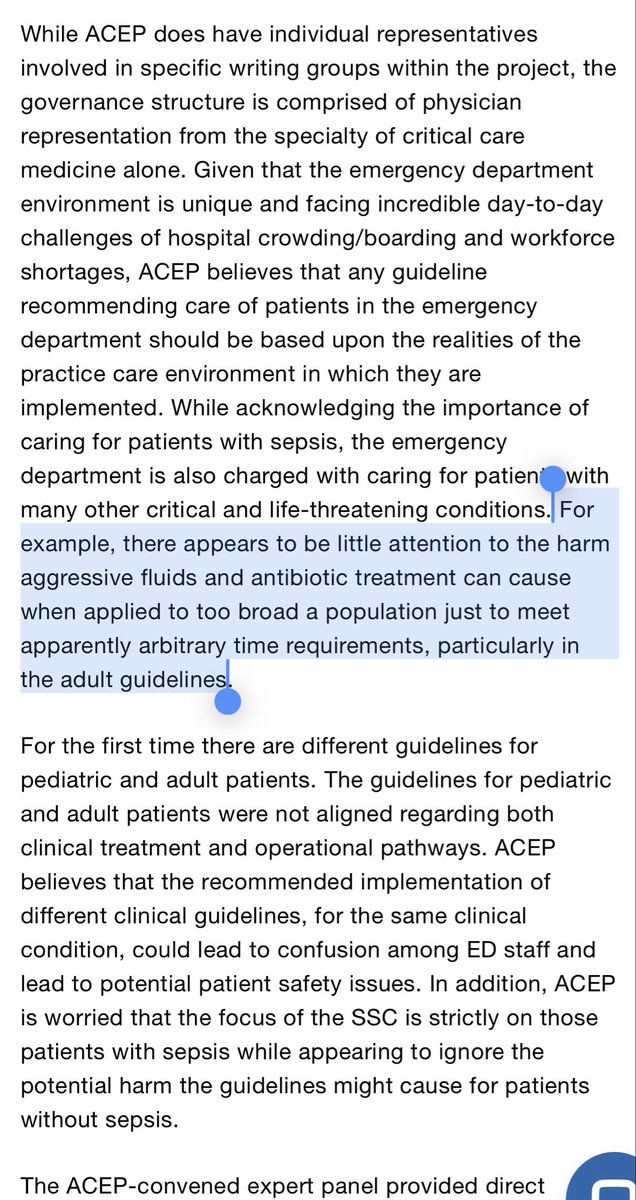
kudos to @ACEPNation for calling out the Surviving Sepsis Campaign 2026 guidelines and not joining in this madness.
ACEP is great at making evidence-based policies that actually *help* provide better patient care.
When ACEP is politely burning your guideline, you’re in trouble.


GIF
English
stefano parlamento retweetledi

Excellent video explaining cardiac axis determination
English
stefano parlamento retweetledi

Rapid explanation : Pathophysiology of Laryngospasm: Part 1
This film explains the pathophysiology of laryngospasm. In part 2 (coming out soon), I’ll explore how techniques (Larson’s manoeuvre & gentle chest compressions) can help relieve laryngospasm. @WWLNHS #medicaleducation
English
stefano parlamento retweetledi
new AHA/ACC guidelines on pulmonary embolism:
similiar to the Surviving Sepsis guidelines
- overall mediocre
- make some nice points
- most folks will accept them because they’re backed by so many societies
- will cause confusion & delay progress
(blog incoming soon)
Edgar Argulian@argulian
A table from newly published AHA/ACC Pulmonary embolism guidelines jacc.org/doi/10.1016/j.… Any comments from echocardiography colleagues?
English
stefano parlamento retweetledi

In the post Andromeda-Shock 2 era, here's how I assess shock:
1. Start with microcirculation
- cap refill
- mottling
- urine output
- lactate
- mentation
If abnormal, there may be a hemodynamic target to optimize.
2. Assess fluid tolerance (aka how likely will my patient be harmed by IV fluids)
- biventricular function, congestion, overload, acute illness, oxygenation status.
3. Phenotype patient's hemodynamics
Quick end easy to start:
1. What is the most likely cause based on history? (e.g. bleeding)
2. Low DBP --> ? low SVR
3. Narrow Pulse Pressure --> low stroke volume
More sophisticated:
1. POCUS for biventricular function and colour on valves
2. VTI (or some stroke volume surrogate)
3. Congestion (if not done in fluid tolerance.
From here, trial different interventions re-assessing cap refill and perfusion Q30min or so.
1. Low SV and normal biventricular function? Consider fluid challenge.
2. Low DBP --> consider vasopressors
3. Poor LV/RV function and low SV --> consider inotropes
4. Bleeding --> blood
How fluid tolerance influences things is that if I have a patient who is very fluid intolerant, even if they may be fluid responsive, I may consider vasopressors to increase their preload (recruit venous capacitance) before jumping to fluids.
Do I follow the andromeda-shock 2 protocol to the letter? No. Does the iterative, microcirculation first approach inform my approach, 100%.
Curious what others do here in the post AS-2 era?
GIF
English
stefano parlamento retweetledi

ECG tools I use teaching cardiology fellows:
1. Cardiac axis simulator → cardiac-axis-training.netlify.app
2. Ladder diagram generator → lewisladder.netlify.app
3. Rhythm simulator → ecg-rhythm-simulator.netlify.app
4. ECG trainer with AI feedback → ekgcases.com
Bookmark this.
English
stefano parlamento retweetledi
Afterload 🧵
The physics of circulation part 5
Afterload is tricky to understand.
It is not blood pressure.
It is not SVR.
It is not “how tight the arteries are.”
To understand it, we need to separate three things that are routinely blurred.
English
stefano parlamento retweetledi

stefano parlamento retweetledi
Why critical closing pressure (CCP) always felt wrong
For years, I found CCP papers confusing — not because the idea of vessel collapse is wrong, but because CCP was often treated as something that exists all the time, as if it continuously governs perfusion in normal, open-flow states.
That framing immediately caused problems and led to some very strange ideas.
CCP was frequently presented as a downstream opposing pressure — something to subtract from MAP. Hence formulas like tissue perfusion pressure (TPP) = MAP − CCP. But a collapse threshold cannot be a back-pressure. CCP is only relevant once arterioles have collapsed.
CCP was also used to explain autoregulation, even though autoregulation occurs in proximal arterioles at much higher pressures than those at which CCP becomes relevant in distal arterioles.
CCP − Pms was then used to describe capillary perfusion, even though a collapse threshold cannot be an input pressure. This is simply a category error. CCP marks the point at which arterioles close. Above that point, flow is governed by ordinary arterial–venous pressure gradients and arteriolar tone — not by CCP.
A waterfall analogy — developed for passive collapsible tubes (veins, zone-1 lung) — was exported into arteriolar physiology. But arterioles are not floppy veins. They possess active smooth-muscle tone, making them functionally open or closed, in a way veins are not. A true waterfall would make venous pressure irrelevant for organ blood flow — which it plainly is not.
And here lies the central contradiction:
If capillary perfusion were governed by CCP − Pms, how could there simultaneously be a “waterfall” in which venous pressure does not matter? The framework collapses under its own assumptions.
From this came papers proposing that we might manipulate — even widen — waterfalls, which would in fact imply closing off more vascular beds rather than improving perfusion. In healthy physiology, there should be no collapse and no waterfall.
None of this fits with clinical observation:
• Raising MAP does not reliably restore perfusion
• SVR does not reliably reflect tone
• Oedema and venous congestion clearly impair organ blood flow
• Monitors can reassure while tissues suffer
The problem was never CCP.
The problem was how it was framed.
Active arteriolar closure was conflated with passive Starling-resistor behaviour.
In reality, CCP is a conditional collapse threshold: vessels are either open or closed. It is not continuously “acting” when flow is normal.
Once those ideas are separated, the contradictions disappear. CCP stops adding confusion and instead explains haemodynamic incoherence.
CCP always felt wrong because it was being asked to do jobs it was never meant to do.
Used correctly, it simplifies physiology — and supports genuinely personalised care.
And that leads to the most important practical point:
What matters clinically is restoring flow continuity across the macro-to-micro interface — reducing excessive tone, relieving external or venous constraint, and avoiding pressure strategies that worsen collapse rather than reopen closed beds.
That is what CCP is actually useful for and why it finally makes sense.
Read our full paper here 👇
@ThinkingCC @khaycock2 @EMNerd_
mdpi.com/2075-4426/16/2…
English
stefano parlamento retweetledi
Our paper is out!
@ThinkingCC @khaycock2 @EMNerd_
We revisit critical closing pressure (CCP) and show why ~50 years of confusion arose — and why CCP has been repeatedly misused as a perfusion pressure, an autoregulatory variable, and a “waterfall” you can manipulate.
CCP isn’t niche. Used correctly, it explains haemodynamic incoherence and guides personalised shock care.
mdpi.com/2075-4426/16/2…
English
stefano parlamento retweetledi
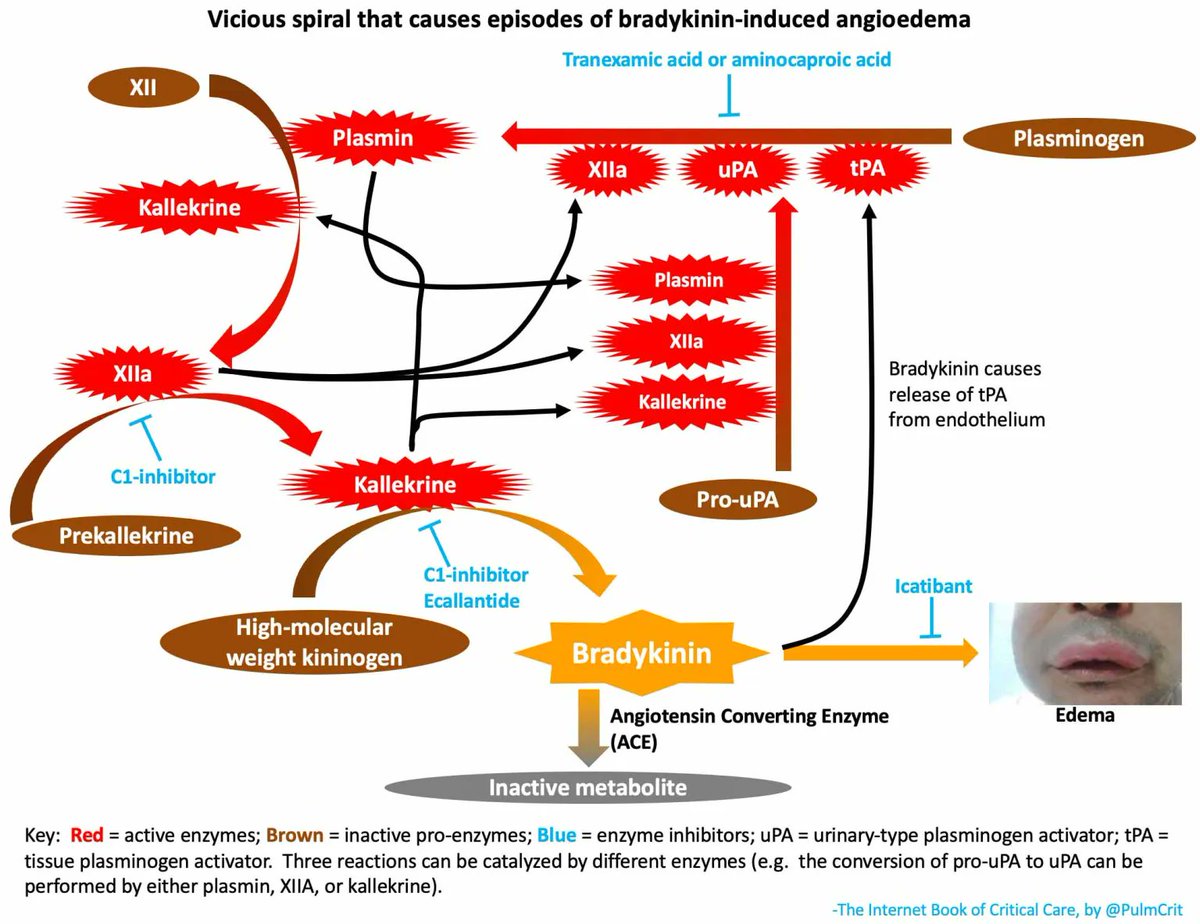
Thrombolytic-induced angioedema is bradykinin-mediated.
Steroids/epinephrine/antihistamines don't seem to be effective. Epinephrine risks causing HTN & promoting intracranial hemorrhage post-tPA with no real benefit.
My approach to this problem is here: #thrombolytic-induced_angioedema" target="_blank" rel="nofollow noopener">emcrit.org/ibcc/ais/#thro…
English
stefano parlamento retweetledi
Pressure 🧵
The physics of circulation part 2
We use the word pressure constantly in medicine (blood pressure, filling pressure, perfusion pressure).
And we usually treat pressure as an agent.
It isn’t.👇
English
stefano parlamento retweetledi
🧵 Thread: Why cardiovascular physiology feels confusing (even to experts)
Part 1 of my 'The physics of circulation' series
Cardiovascular physiology isn’t confusing because it’s complex.
It’s confusing because we routinely mix up description with causation. And our language subtly reinforces the error.
English
stefano parlamento retweetledi
#Mondaytip
🧠 New @American_Stroke #Stroke Guidelines
✔️ TNK = first-line option for IVT
✔️ EVT expanded (large cores & basilar ≤24h)
❌ No aggressive BP or glucose lowering
👶 First pediatric AIS guidance
⏱️ Systems of care matter more than ever
doi.org/10.1161/str.00…

English
stefano parlamento retweetledi
🧵 Why can oxygen worsen respiratory failure in COPD?
Many clinicians still fear giving oxygen to COPD patients.
The reason they’re taught?
"Loss of hypoxic drive"
But this is mostly a myth.
Here’s what really causes oxygen-induced hypercapnia 👇

English
stefano parlamento retweetledi

This is a big deal. Frequentist statistics have done a lot of damage to medical science. People rely on P values without really understanding what they mean. Many faulty conclusions have been made because of them.
Once you understand Bayes methods, you’ll never rely on frequent tests again. Bayes methods are completely aligned with clinical thinking and should be the standard methodology used for statistical analysis in clinical research.
Frank Harrell@f2harrell
This is a big step forward in improving the efficiency of clinical trials of drugs and biologics, and a big day for @US_FDA which I've been dreaming of for decades : fda.gov/news-events/pr… #bayes #RCT #clinicaltrial #pharma
English
stefano parlamento retweetledi

EMCrit 416 - JanuAIRWAY - State of the Airway 2026
-Difficult Airway Assessment
-PreOx
-Med Choices
-eFONA
Let's reestablish our intubation foundations by using the new DAS guidelines as a guide to discussion...
emcrit.org/416

English