@icefordinneryum @Biohazard3737 Elaborate way to say that there’s an efficient market
English
pharmakopios
71 posts









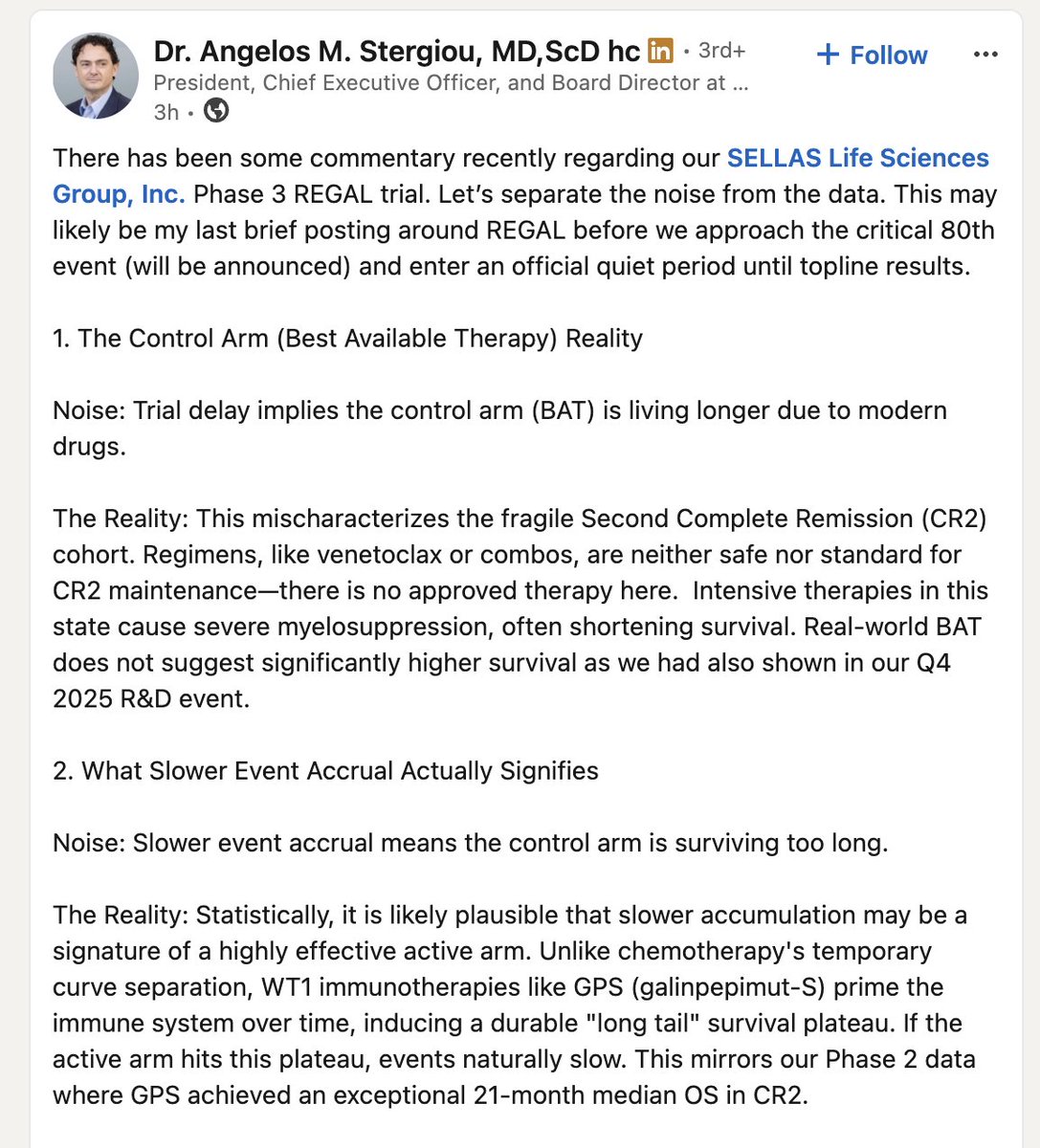
How is it possible that $SLN never released any data from GEMINI-II


$SRPT First person who can tell me all the things wrong with this slide gets a cookie. Slide 10. investorrelations.sarepta.com/static-files/7…