rajEndiran retweetledi

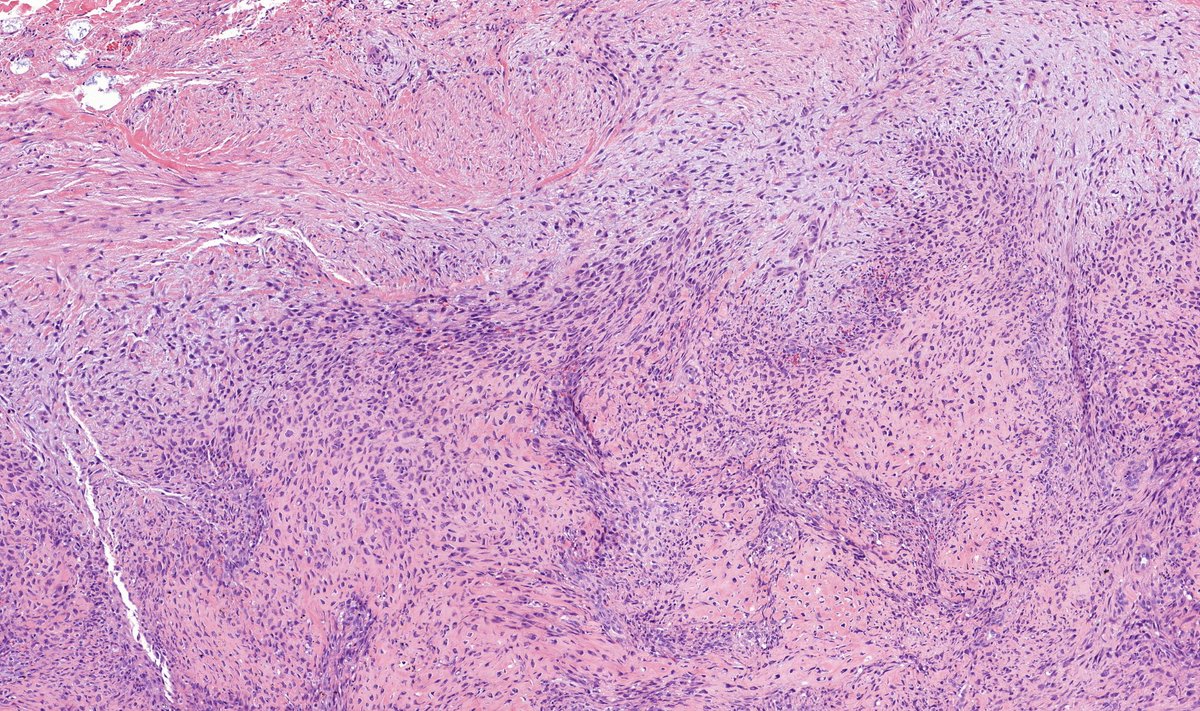
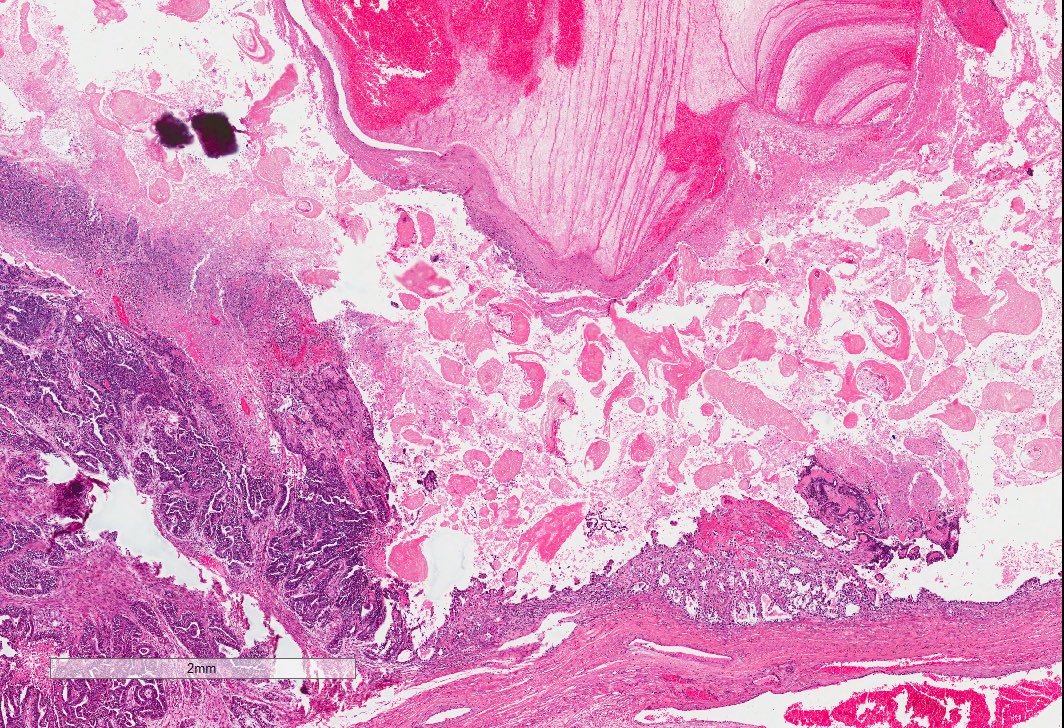
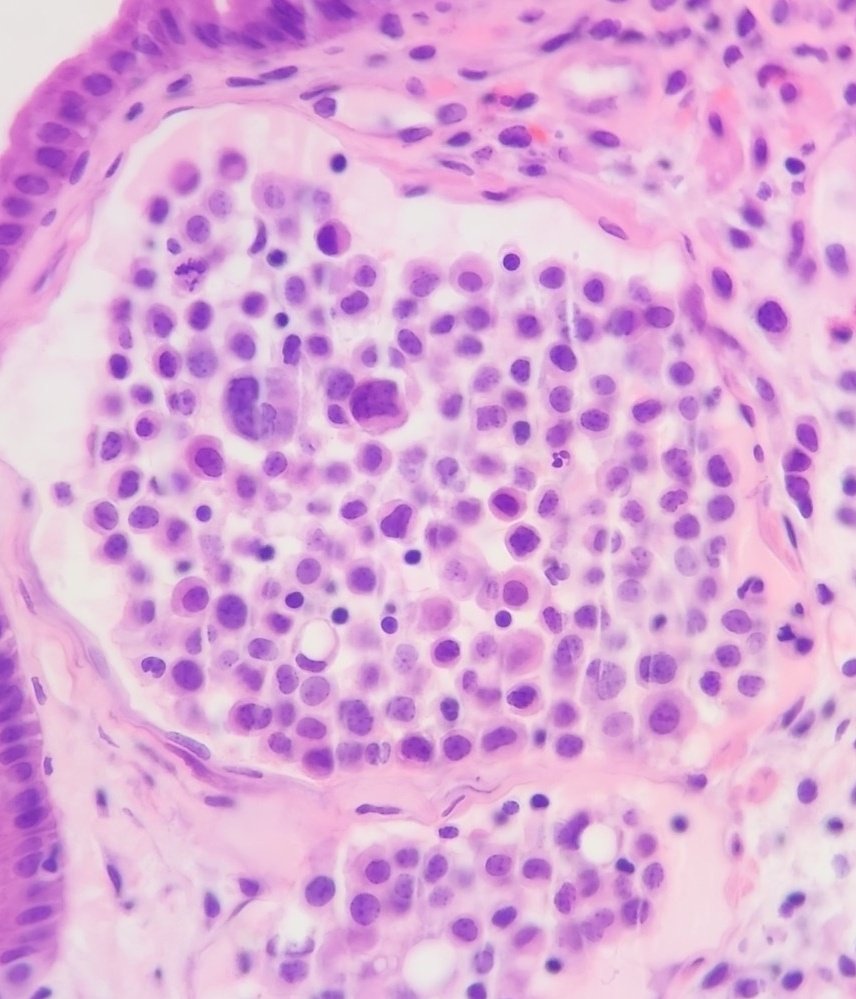
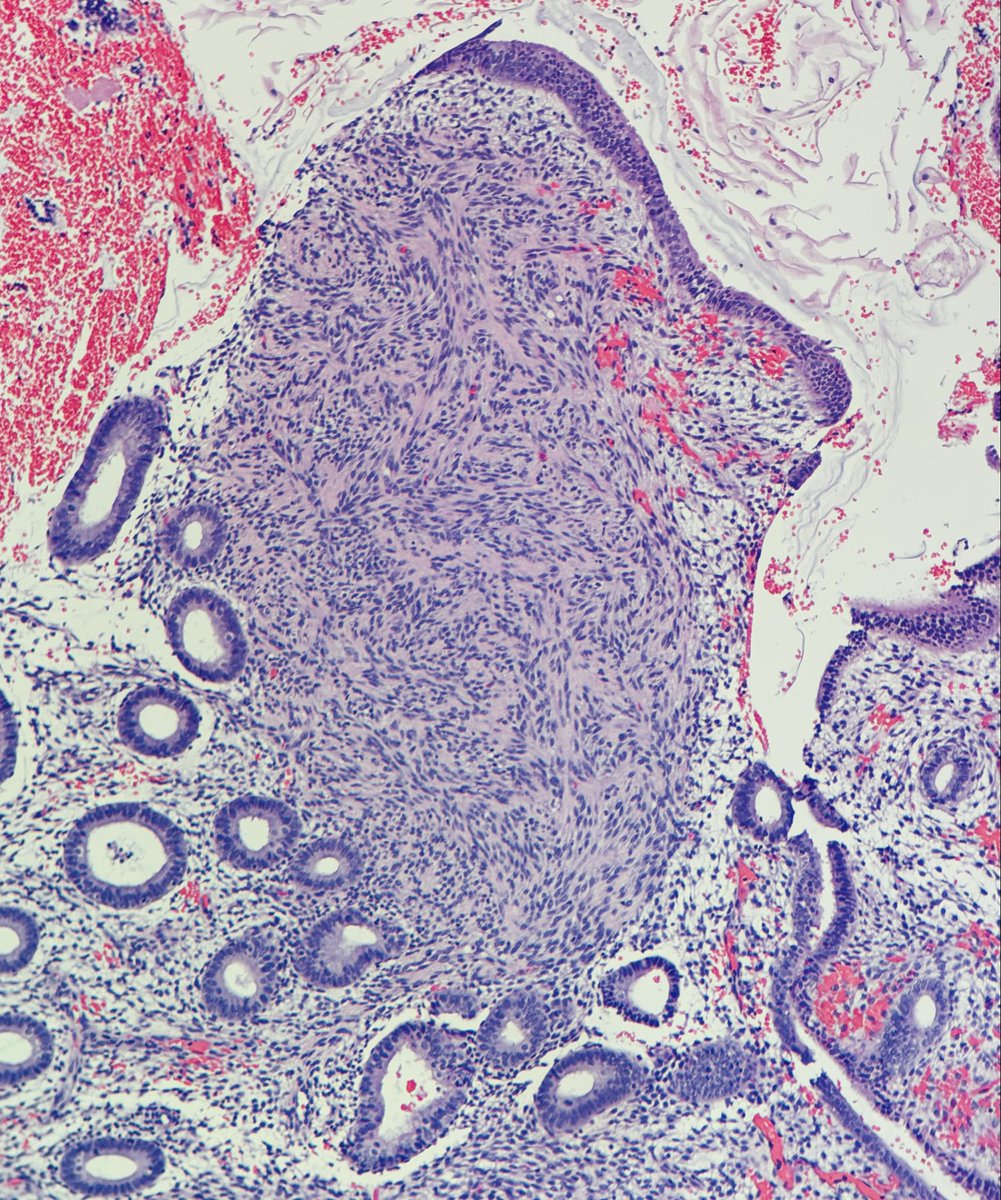
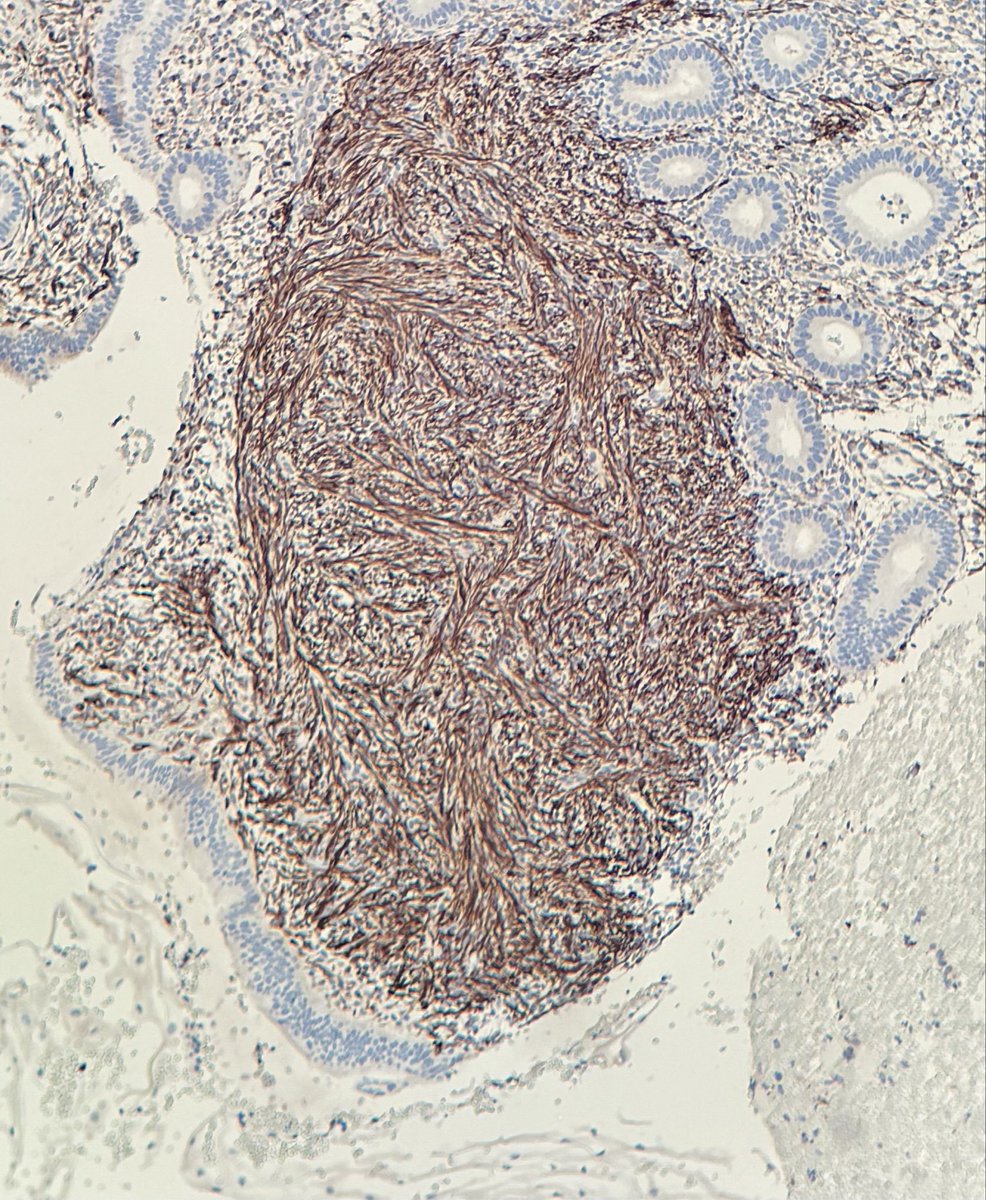
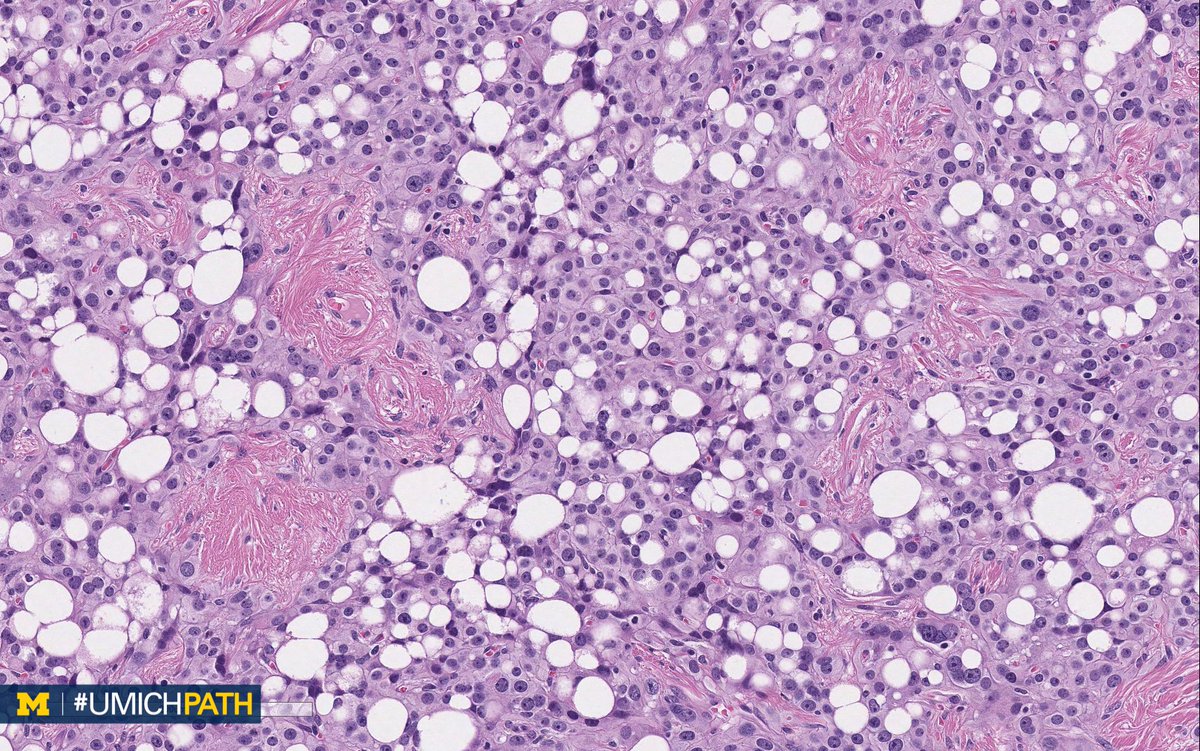
A young female with progressive shortness of breath and dry cough
🩻 diffuse B/L ground glass opacities
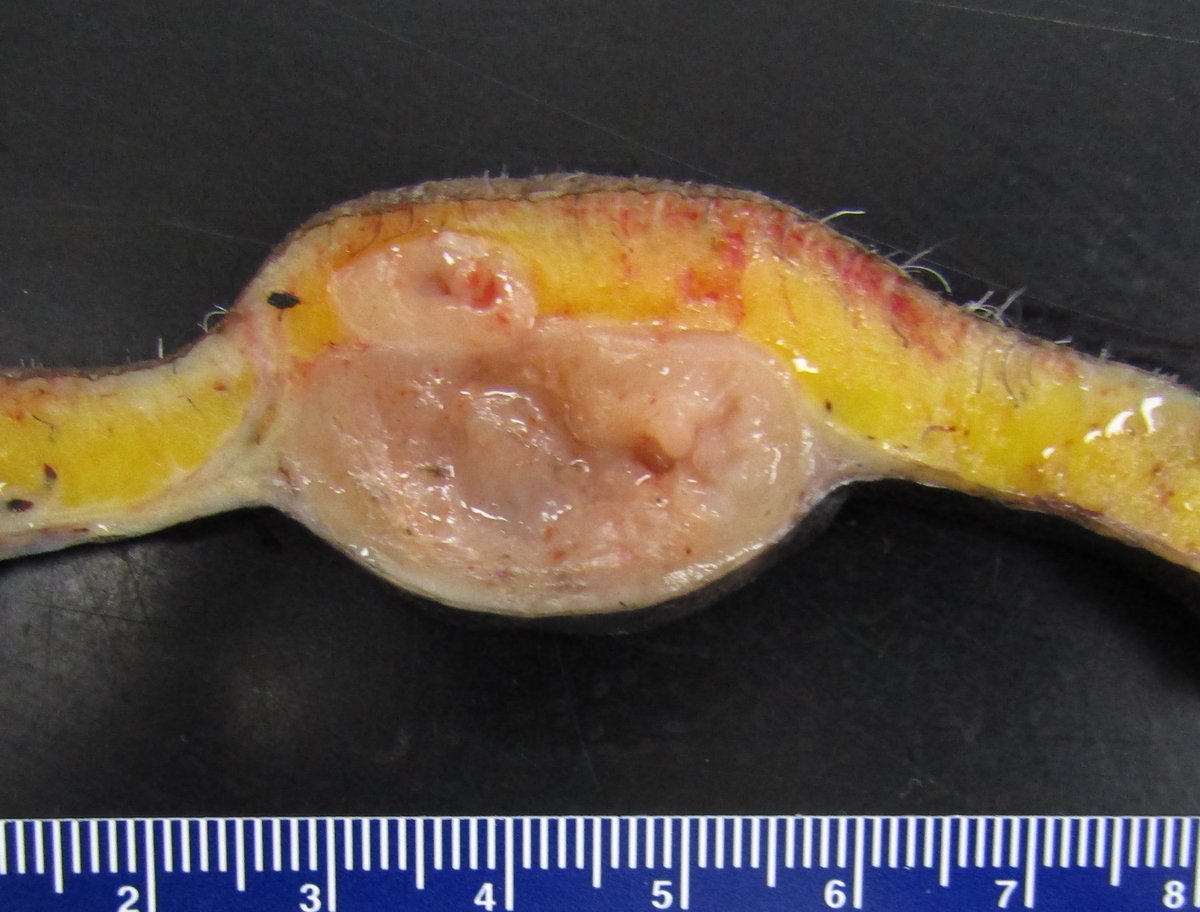
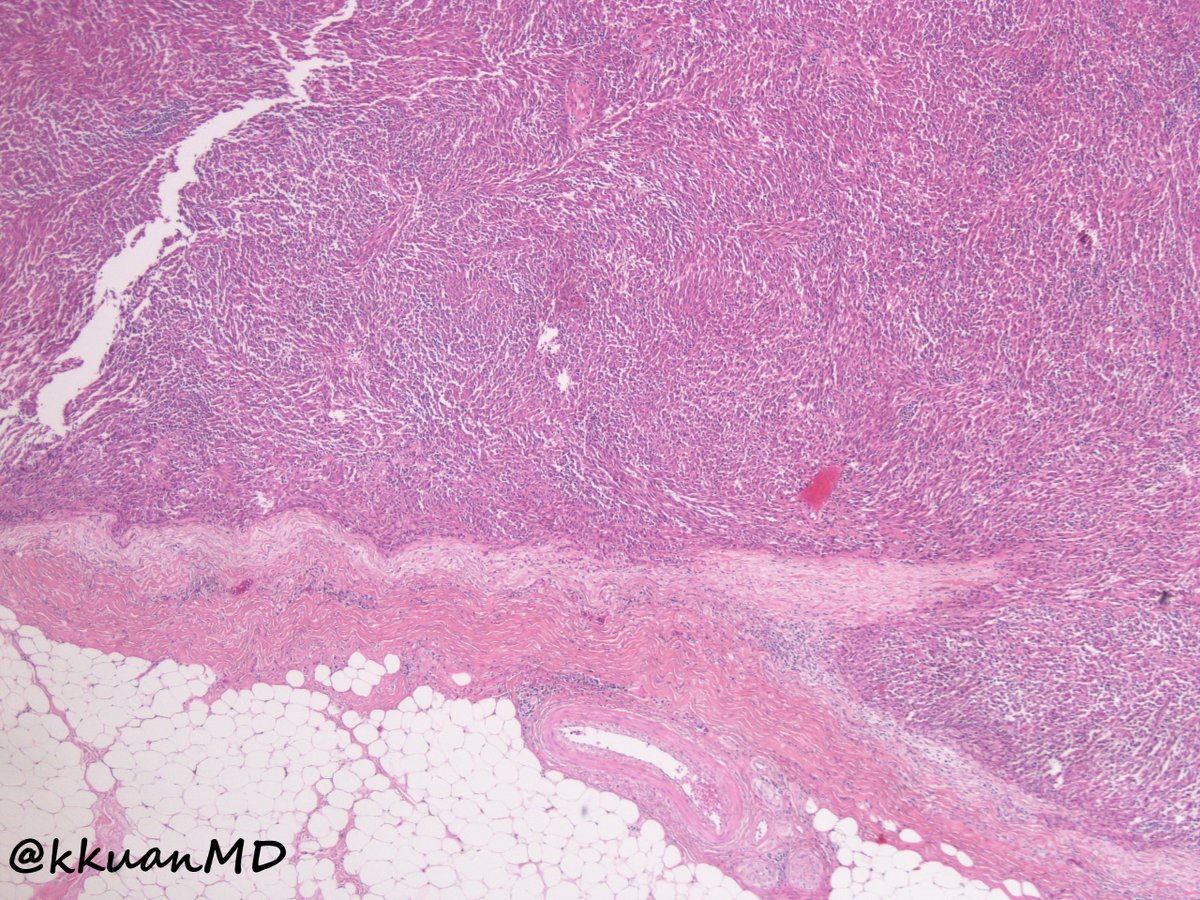
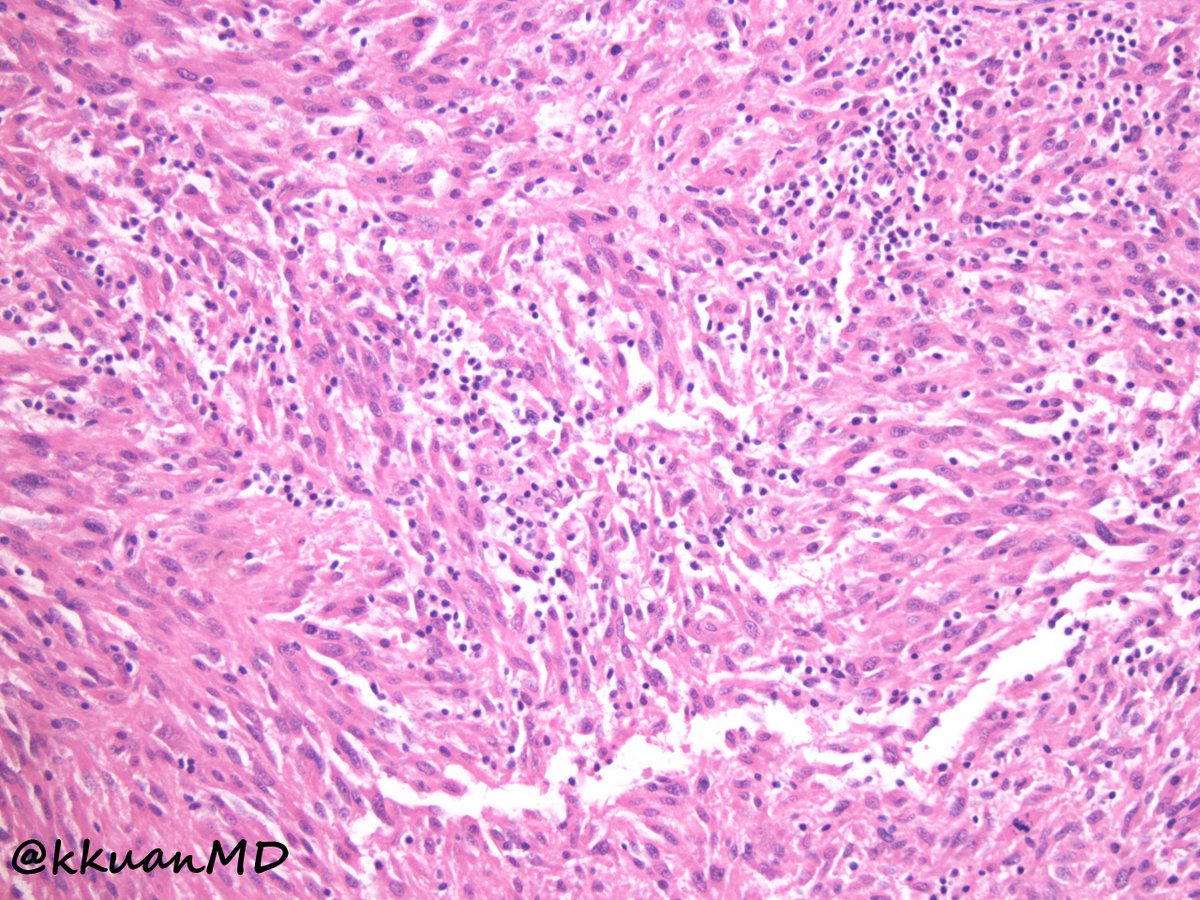
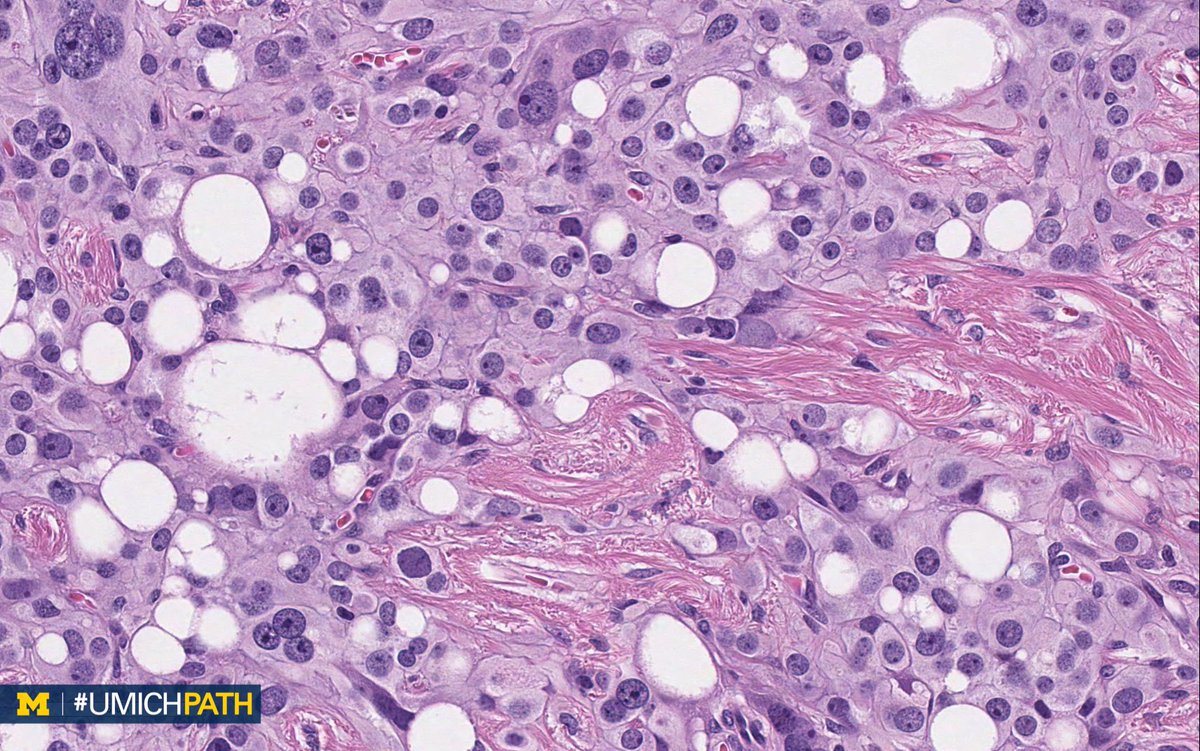
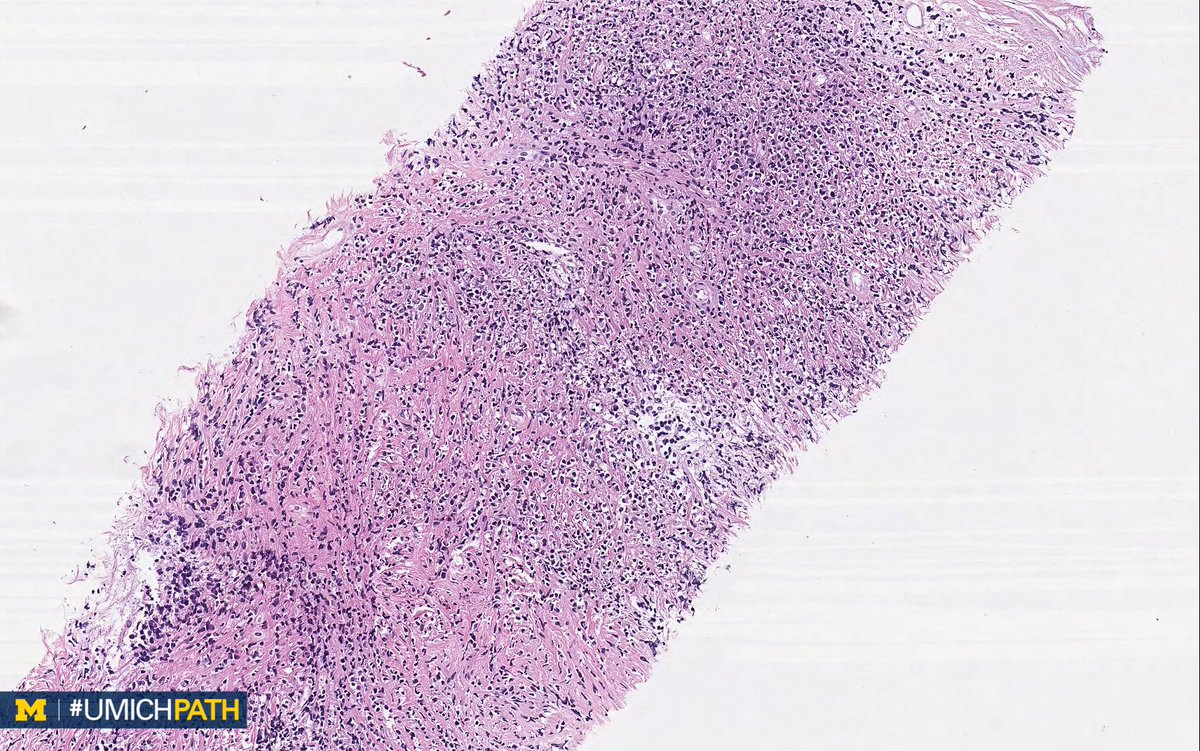
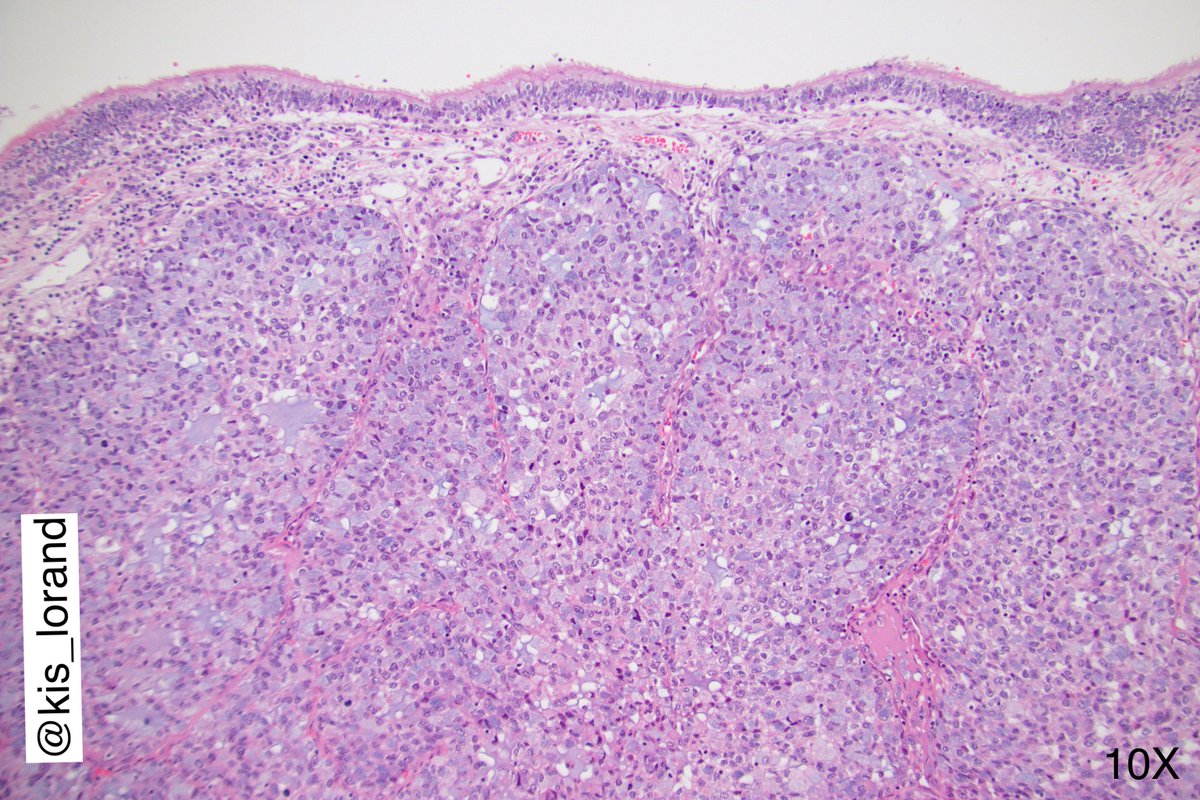
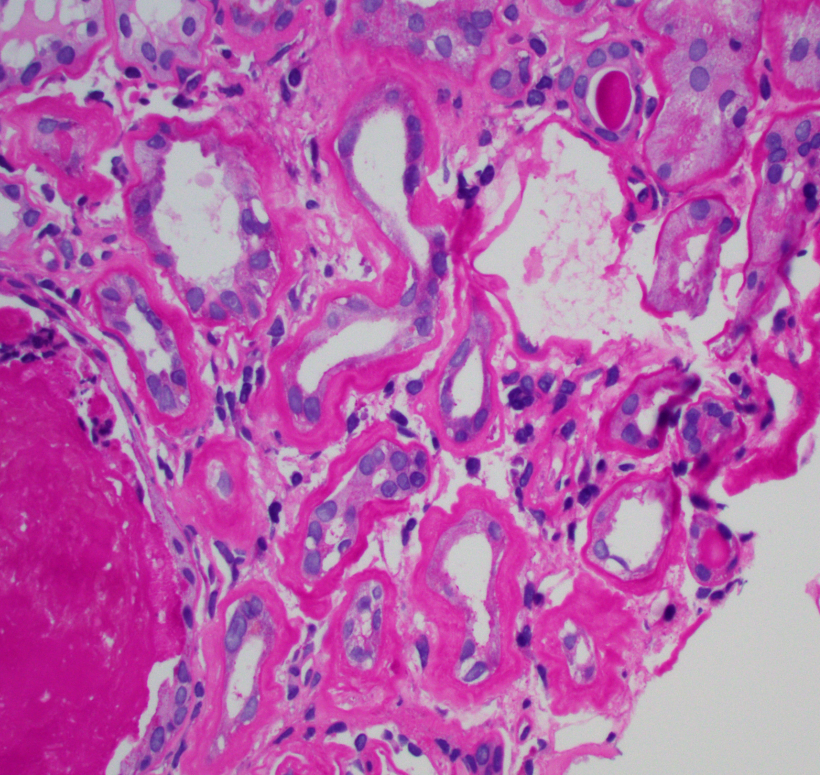
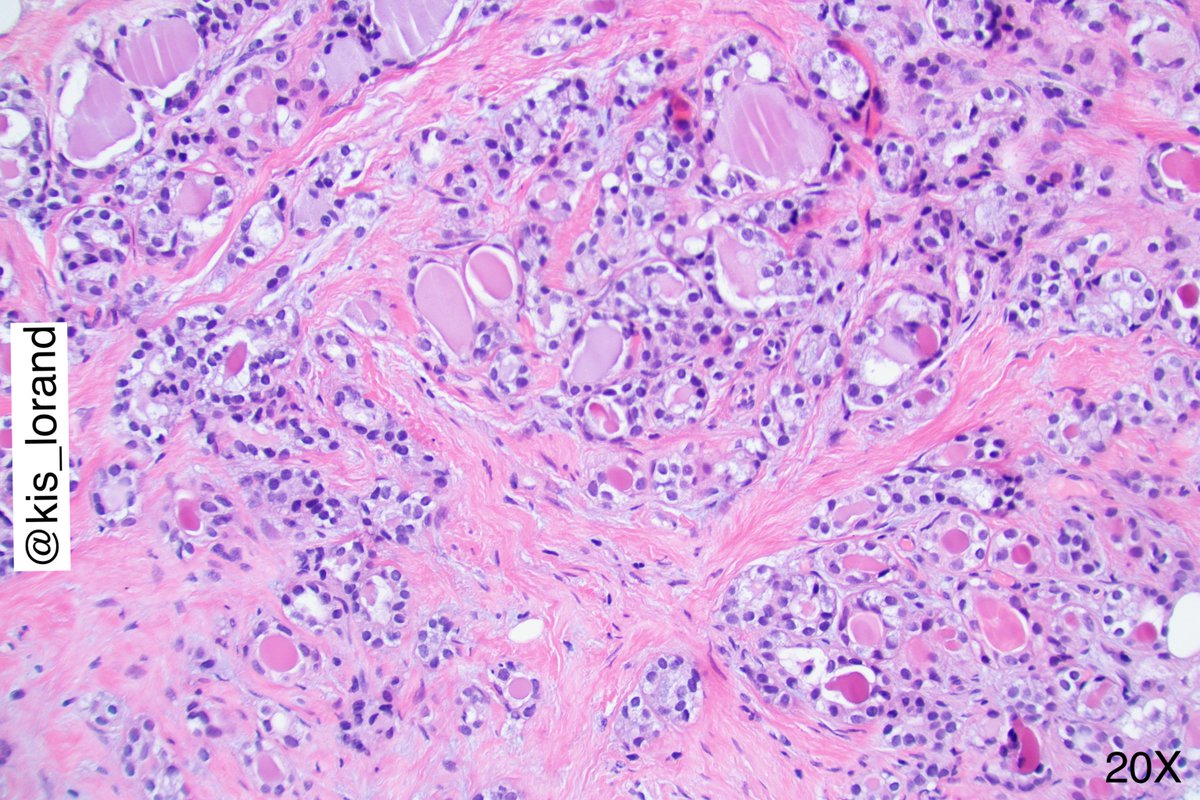
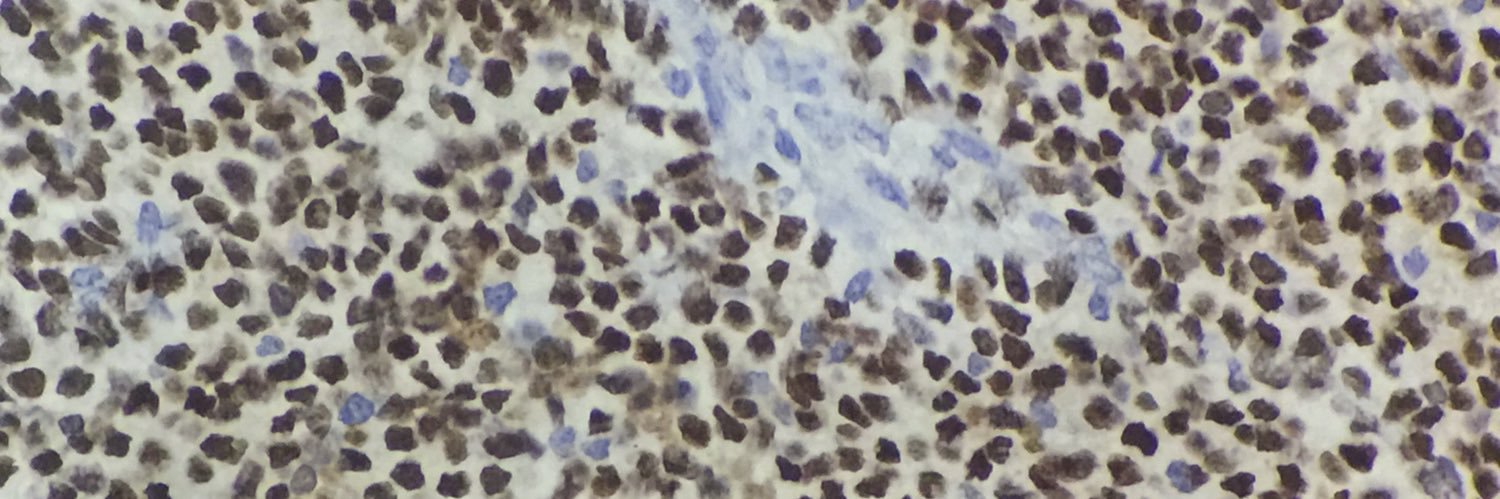
Here is the biopsy from the lung.
#PathTwitter #MedTwitter #PulmPath #PulmPathFellow

English
rajEndiran
4.4K posts

@rdpatho
Visiting Prof. Of Pathology, Sri Ramachandra Institute Of Higher Education & Research
2026 Yıllık Özeti
@rdpatho hesabının Twitter yılını gör