RSanchezEndo retweetledi

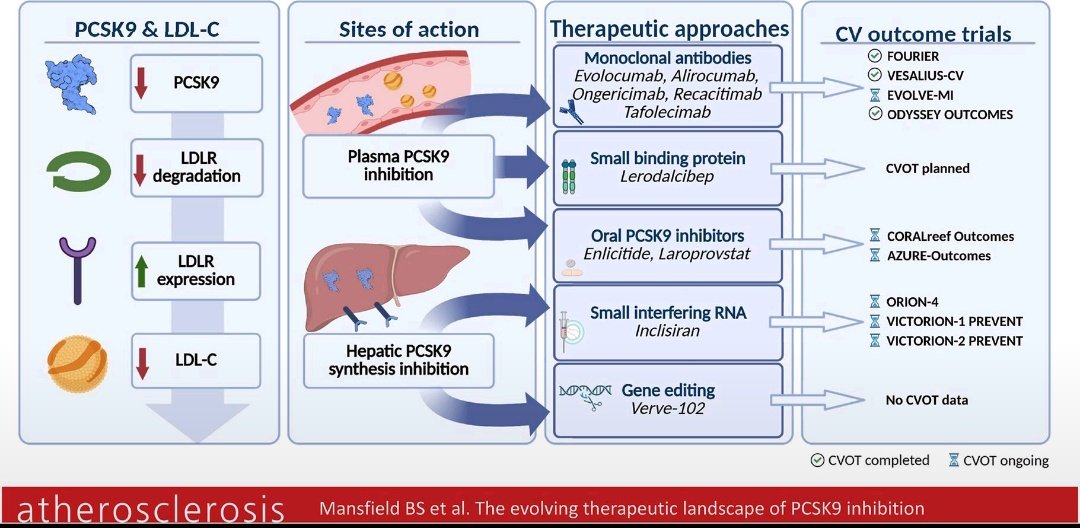
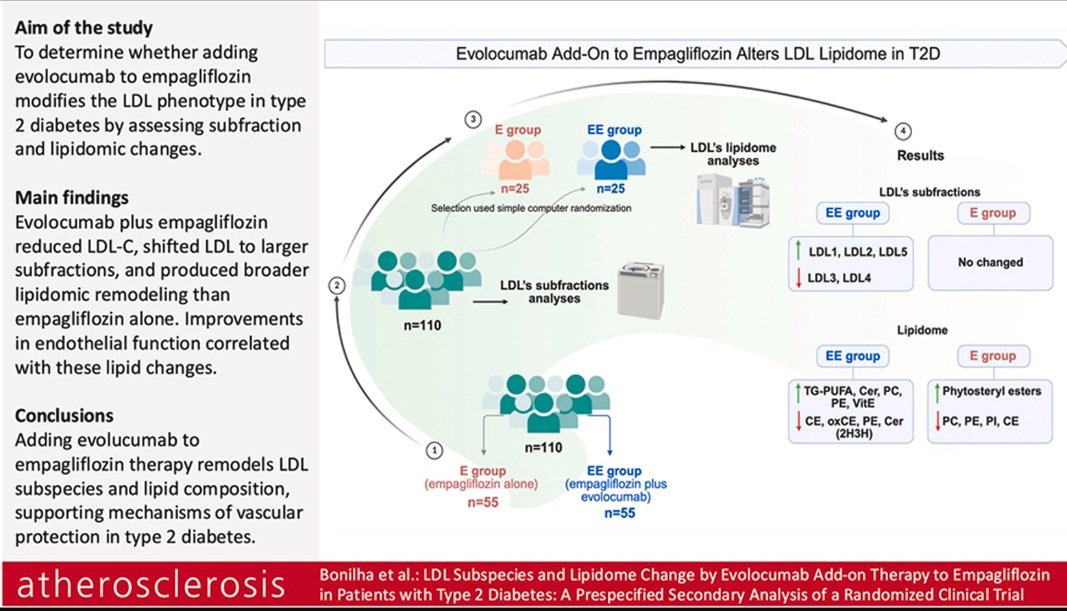
✅Adición de inhibidores de PCSK9 a la terapia con inhibidores de SGLT2
➡️Provoca una remodelación de las subespecies de LDL y de la composición lipídica, con implicaciones mecanicistas para la protección vascular en la diabetes tipo 2.
atherosclerosis-journal.com/article/S0021-…
Español