@NikhilShahMD Dr Shah failed to mention this was recorded fortuitously when transcutaneous pacing was interrupted briefly for a rhythm check in the ER. He saved the patient with a temp wire
@Ed_Gerst I agree it’s probably biatrial jumping from LA to RA across BB. These can be tough to get but we’ve had success targeting the latest site in anterior LA before it crosses BB to RA
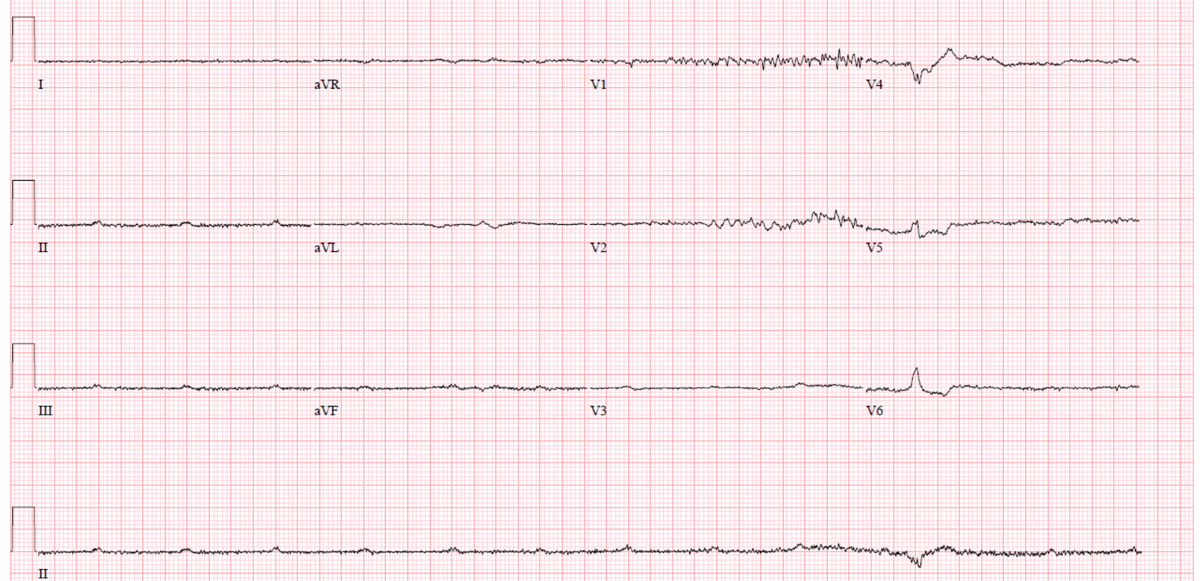
1. Interesting case #EPEEPS showing the down side of the anterior line for MA flutter. Pt underwent ant line for MA flutter at OH and then developed incessant slower flutter with similar morphology. Is this still MA flutter?
@FYang_EP 3x8mm balloon. Volume was upper limit of what I had seen published. Vein was also long enough to allow separate injections at multiple levels
Redo persistent AF after PVI. Veins are quiet (right image). On left, note massive voltage attenuation after vein of Marshall alcohol ablation. No RF delivered!
@FYang_EP What I didn’t show you was that this was the largest VOM I’ve ever seen, over 3mm in diameter and we injected 12cc of alcohol. This was not the typical case but was so profound I wanted to share
Congratulations to Lahey Cardiac Arrhythmia Service team for receiving first in Massachusetts ACC Electrophysiology Accreditation. Credit goes to EP Lab Director Muqi Chaudhry MD and lab nurses Anna and Bing. #ACC#LaheyEP
Redo AF and enormous CS due to persistent left SVC with figure of 8 reentry in CS. Small circuit present on proximal roof connects to a 2nd loop traveling prox to distal and then returning along floor. Terminated with ablation on proximal CS roof
@Dr_Santangeli@AbbottGlobal Nice case and supports the Bordeaux group’s recommendations at the AF Symposium last week that we get back to PVI, roof and MI for persistent AF. Just need better tools for permanent lesions!
Dual loop LA flutter (MA and roof dependent) mapped with #HDgrid, confirmed with 4-site entrainment and ablated with #TacticathSE. Great ablation platform - huge step up in handling, steerability and tracking @AbbottGlobal
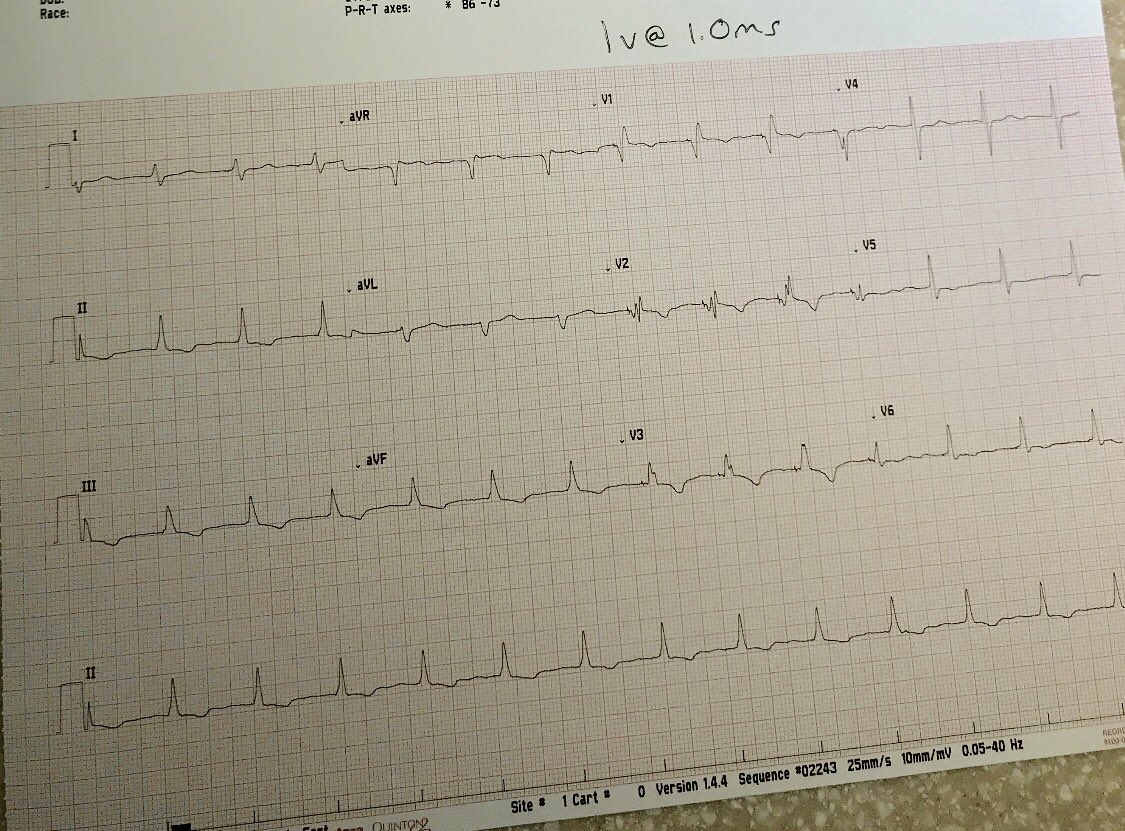
72 yo m Severe AI s/p AVR, perm AF and high degree AVB. Sent for leadless. Found this. Tried HBP and no luck. Then moved the lead caudally. Narrower QRS when compared to RV pacing. Ideas?
#EPeeps#dontdisthehis
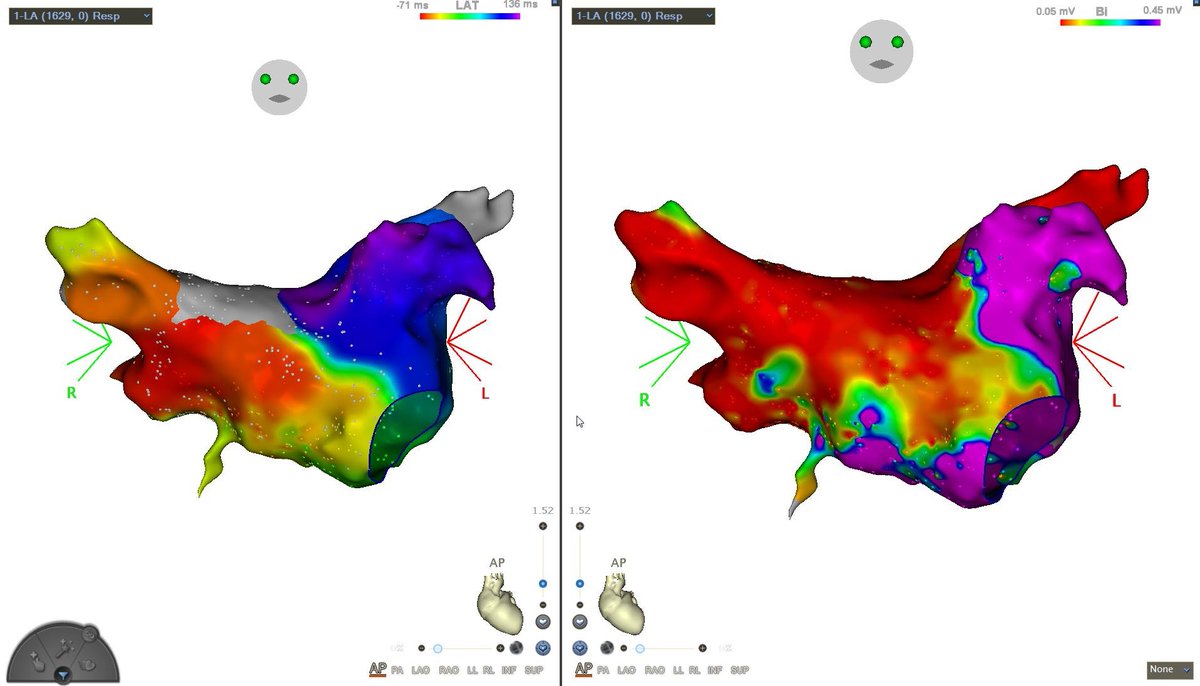
@mustafa_omarov@w04f40 SVC/RA junction terminated AT immediately. After ablation we paced RA and documented block across Bachmann’s bundle with LA activation up CS and across LA lateral to medial
Redo AF ablation with durable roof and anterior line during biatrial AT. Note the delay as the wavefront comes across the anterior LA from lateral to medial. Then early activity in SVC/RA junction as impulse uses Bachmann’s bundle to jump to RA. Down septum and up mitral isthmus
Single lesion at SVC/RA junction terminated AT to sinus. I’ve noticed in a few of my old reports that the final AT in a complex case was “focal AT” from SVC/RA junction. I think this type of biatrial AT is more common than we think