🔥BREAKING: FASTEMI is out!
POCUS changed management in 14% of STEMI cases + 97% NPV for mortality. Fast, reproducible, no delay to PCI.
Huge honor to work with @Babar_Basir and all our amazing team!
@SCAI @EAPCIPresident @PCRonline
André B Amon@AndreAmonMD
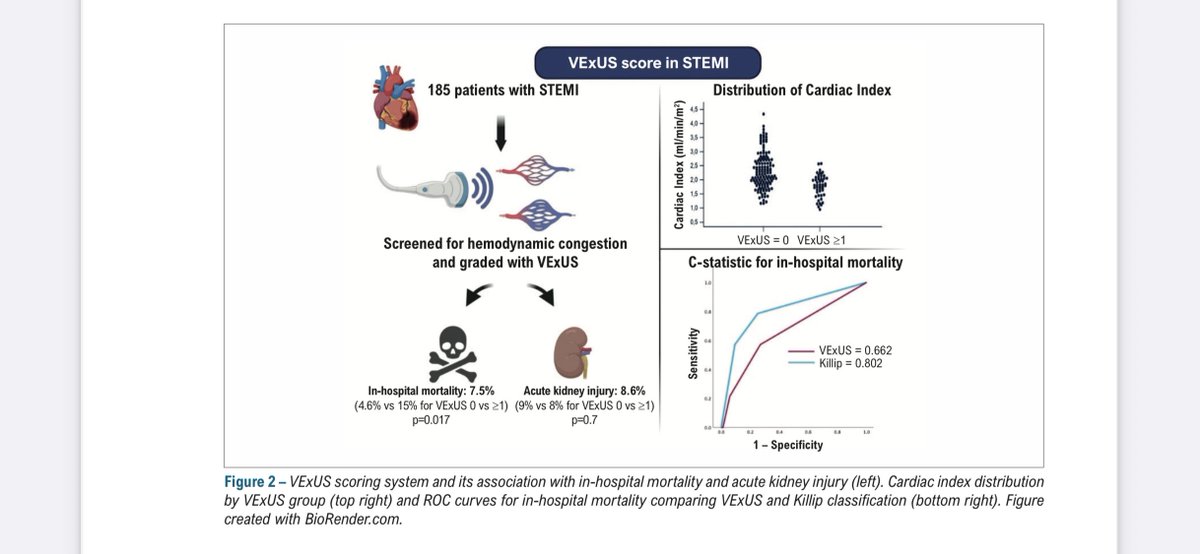
Our FASTEMI study is now published! 🎉 This quick and practical POCUS protocol in STEMI can be truly decisive: it guides management, identifies critical differential diagnoses, and achieves a 97% negative predictive value for in-hospital mortality. rdcu.be/eRSkX
English