ทวีตที่ปักหมุด
Jon Coe
2.8K posts


Jon Coe
@coezycoe
mid-wit-certified by wife, Little League Coach, MIT baseball turned Giants/Cardinal homer, inventor 10^2+, CEO @ https://t.co/5Nyr8kezJX
Bay Area / Aspen เข้าร่วม Temmuz 2009
1.8K กำลังติดตาม521 ผู้ติดตาม
We are so cooked as a society. Everyone saying it's AI these days, but 4 lag screws did the trick.
🌵 RC | The Nostalgia Pro🕹️📺@NostalgiaPro
I hired a local pro to handle the mounting. He quoted $250, I gave him $300. He showed up fast, brought a second guy, and did a flawless job. A lot of people in the replies completely missed the point. This was never about the physical act of hanging a TV on a wall. It was about paying for a service that a massive retailer simply refused to fulfill. @BestBuy took the money and walked away from the job. They will never see another dime from me.
English

For those that want the robotic strike zone. That pitch last night would definitely have been a strike. All it would have to do is touch any part of the 3d cube. And with breaking balls you could throw some that bounce. Yes literally bounce that would clip the cube and be called a strike. So as a reminder. It’s not where the catcher catches it. It’s where the ball crosses the plate. I promise the robotic strike zone Would have that as a strike because it would have crossed let alone clipped the strike zone cube.
English
@endingwithali He turned into a great, well adjusted dude, dad, and husband in due time. Everyone has their own finishing school deficiencies 😉
English

my mom made it a point when i was growing up to immerse me in the arts, knowing i was going to be a third gen engineer.
broadway shows, art history, travel often. museums, learn the greats, reading of any kind (i literally would inhale archie comics growing up)
MIT also understood the importance of balancing engineering and humanities. you had to take a minimum number of HASS (humanities, arts, social sciences) credits, which equated out to basically be 1 class a semester. it forced you to be outside of your engineering specialty.
to succeed in life you have to be well rounded. you need to be able to have conversations with everyone, you need to be able to appreciate things outside of your captialism.
taste isnt just what looks good together - its understanding social scenarios, knowing how to exist in different spaces, and being able to connect with anyone.
engineering, founding, and business cannot exist without the arts. the arts are what give you taste.
Michael J. Miraflor@michaelmiraflor
Sound the alarm. The VCs are now publishing essays about the value of Brand. The “taste” bros will follow suit.
English

Crazy that one company alone accounts for 5% of this number
CNBC International@CNBCi
U.S. payrolls unexpectedly fell by 92,000 in February; unemployment rate rises to 4.4% cnbc.com/2026/03/06/feb…
English
@RobertStock6 Great work dude--the best part for the game is we'll start to see new metrics from players' unique insights. Might even nudge negotiations in favor of MLBPA 😉
English

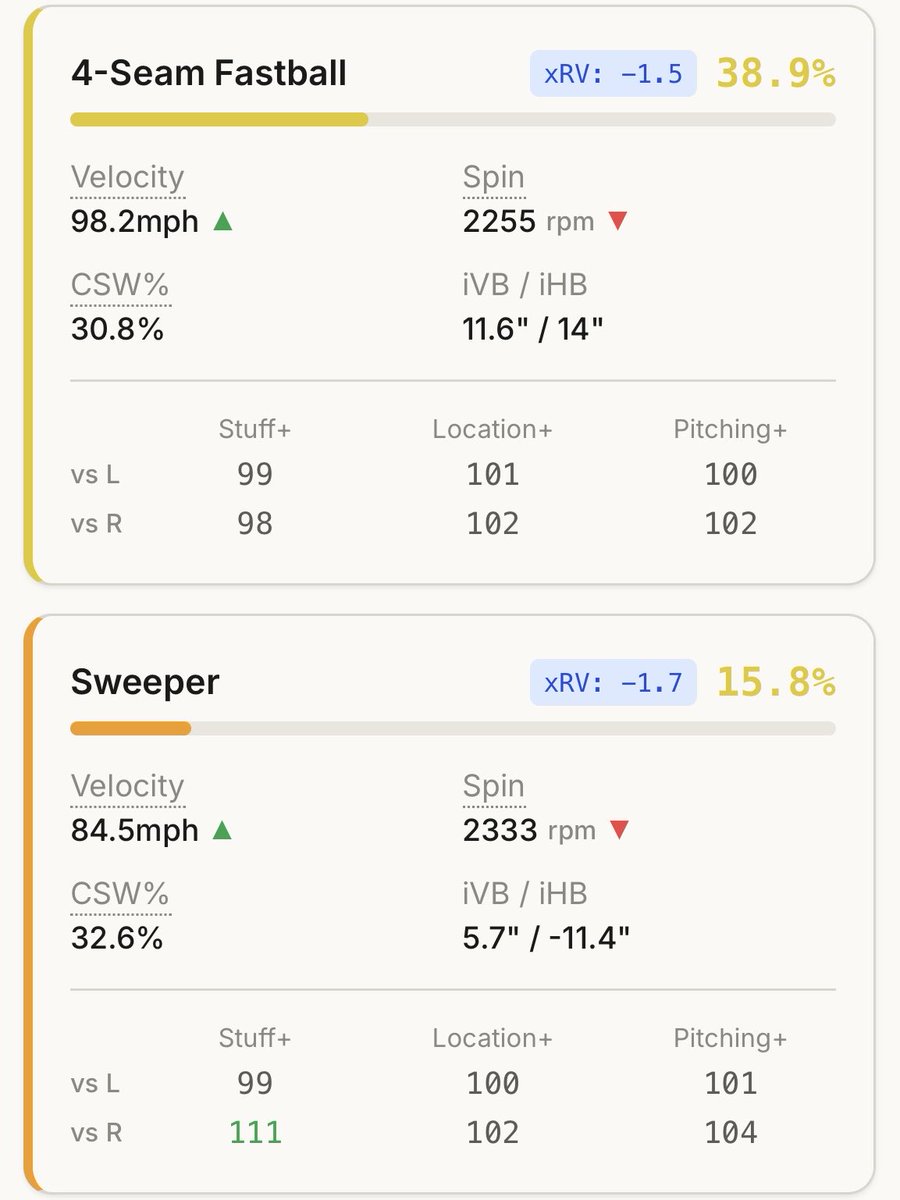
I’m a baseball player. I’ve never written a single line of code in my life.
But over the last few months, I used AI to build a pitching analytics platform from scratch.
8.9M pitches. Custom ML models. Total transparency.
Here is a look at what happens when you give an interested athlete access to AI:



English
This is awesome. Exactly the kind of democratization of tech I've long hoped for. AI for coding, 3d printers are just about there--it will be the everyman's Renaissance, if you can dream it you can build it! Proud a Met is leading the way here.
Robert Stock@RobertStock6
I’m a baseball player. I’ve never written a single line of code in my life. But over the last few months, I used AI to build a pitching analytics platform from scratch. 8.9M pitches. Custom ML models. Total transparency. Here is a look at what happens when you give an interested athlete access to AI:
English
@DrDiGiorgio We used to joke with our surgeons--"you get one nice thing / year, plz choose us." Innovated for 20 years in surgery, hope not to see the inside of a hospital the next 20!
English

Innovative environments where surgeons get to use cutting edge technology on patients to improve both outcomes and surgeon quality of life are great and all….
But have you tried working at a hospital where you’re treated like a burden and asking for basic necessities gets you scolded?
A.T. Mameghani, MD 🇨🇭🇺🇦🇮🇱@atmghn
working in an innovative environment means that you can never lean back and stay calm for one or two years. It's always moving forward. Change is everywhere. Re-dos of trainings, new things rise up quarterly and when you just think, you made it, the software update forces you to go back to the start and re-learn everything. Don't underestimate this, when you invest money in a solution "that makes the surgeon’s life easier"!
English
@nickmmark @IQSURGICAL Wrong IQ Surgical, but check out what Jay Park and Rich Timm are up to
English
@nickmmark Way longer than 3 years to FDA approval even if all the first and last mile problems were solved today. And you're right about everything else. But there are some cool real projects like @IQSURGICAL coming down the pipe in this direction
English

This guy is such a dope.
Ignoring the obvious fact that surgeons already use robots & have for decades, even if the tech to automate this existed *today* it would take 3 years just to study it and get it FDA cleared.
Another obvious point is form factor: the ideal surgical robot isn’t going to be humanoid. It’s much more likely to resemble a spider (aka Davinci) than C-3PO.
The bigger issue is the AI: The reality is that performing procedures is a long tail problem that makes autonomous driving look easy. Optimus can’t even do simple tasks like read the instructions and assemble a Lego kit autonomously.
Autonomous robot surgeons are *FAR* more than 3 years off.
Dustin@r0ck3t23
Elon Musk just put an expiration date on the medical profession. And he gave it three years. The interviewer asked when Optimus would be a better surgeon than the best surgeons on Earth. Musk didn’t hesitate. Musk: “Three years. I’d say three years at scale.” Not a prototype. Not a lab experiment. At scale. To understand why that timeline is plausible, you have to understand the fundamental problem with human medicine. Musk: “Takes a super long time to learn to be a good doctor. And even then, the knowledge is constantly evolving. It’s hard to keep up with everything.” Musk: “Doctors have limited time. They make mistakes. How many great surgeons are there? Not that many.” That is the brutal reality of the greatest healthcare system humanity has ever built. It runs on exhausted humans with biological limits, trained over decades, who can only operate on one patient at a time. Optimus has none of those constraints. It doesn’t get tired. It doesn’t forget a study published last week. It doesn’t have an off day. It doesn’t have a caseload limit. And once you train one, you can manufacture ten thousand more with identical precision. Musk: “At that point, there will probably be more Optimus robots that are great surgeons than there are on Earth.” Think about what that actually means. The scarcity of elite surgical skill has been one of the defining limits of human healthcare since the beginning of medicine. Geography determined your odds of survival. Zip code determined your access to expertise. That bottleneck disappears overnight. Because you can’t train human surgeons fast enough to meet global demand. But you can manufacture infinite robots running identical perfect code. The most valuable skill in the world is about to become software. Infinitely replicable. Infinitely scalable. Available to every human being on Earth regardless of where they were born. Medical scarcity doesn’t fade gradually under that reality. It ends. And whoever controls that code controls healthcare access for billions. For all of human history, the leading cause of preventable death wasn’t disease. It was the shortage of great people to fight it. That problem has a solution now. And it ships in three years.
English
@yanatweets You were at d.school back in the day (very bad Tahoe seasons around that time)
English

@coezycoe I didn't really race growing up and there's something about snow that made it feel safe. As an adult, I now know that it was completely unsafe regardless.
English
When did ski helmets become a thing?
I grew up skiing in the Alps. No one wore helmets.
This winter, I skied for the first time in a decade.
One thing that stood out: not a person without a helmet.
When did that become the norm?
Or is this just Bay Area folks protecting their brains 🙃

English
@yanatweets Agreed felt the same, finally ended up being the only dude on a guys trip without one in my 20s and relented/never went back (plus dad needs to see examples!)
English

When I was 7 years old I was asked by my father what went into the price of a sandwich. Considering it carefully, I answered.
The lettuce, the tomato, the bread and the meat.
I did not consider correctly. I was short quite a few costs as my father was eager to point out. I had forgot the labor of the worker, the rent of the land, the marketing costs of the chain. I wasn’t seeing the full picture.
Today we are all making a similar mistake with AI. We are not considering what cannot be considered. As foreign to the 7 year old as these excess charges were, so are the downstream affects of AI.
In 1850, if you had told a teamster that his horse and carriage would soon be obsolete, he would have envisioned a world of mass starvation for men of his skill. He could grasp the concept of a faster carriage, but he could not conceive of the interstate highway system, the suburban real estate market, or the roadside motel industry. These were not just new products; they were an entirely new social architecture.
We are currently in the teamster’s shoes. We see AI automating the ingredients of our current economy—the writing, the coding, the data entry—and we fear the void. But history shows that humanity doesn't fall into the void; it builds a floor over it.
Karl Marx looked at the dark satanic mills of the 19th century and saw a terminal point. He argued that as the means of production became more efficient, capital would consolidate and labor would become a worthless commodity. He believed capitalism would eventually eat itself because it would run out of things for people to do.
Marx was wrong because he viewed human utility as a fixed pie. He didn't understand that technology doesn't just subtract labor; it changes the nature of what we consider valuable.
When the mechanical loom made fabric cheap, we didn't stop buying clothes. Instead, we invented the fashion industry. We created brand management, retail psychology, and textile engineering.
We moved from a world where everyone owned two outfits to a world where millions of people are employed in the cycle of seasonal trends.
In the age of the steam engine, "handmade" was a sign of poverty. Today, it is a luxury. We are already seeing a shift where the human touch—the artisanal, the face-to-face, and the physically present—is becoming the high-margin sector of the economy.
Every time we automate a simple task, we move the human to a more complex one. We didn't stop needing accountants when Excel was invented... we simply started asking accountants to perform much more sophisticated financial modeling.
The 7-year-old misses the rent and the marketing because they are abstractions. Similarly, we struggle to see the jobs of 2040 because they rely on problems we haven't even encountered yet. We might see the rise of Personal Data Stewards, who manage the interaction between our private lives and public AI models, or Reality Architects, who ensure that the virtual spaces we inhabit are psychologically grounded.
The world works itself out because humans are fundamentally restless. We do not tolerate a vacuum of purpose, we seek higher function always.
English
@ChrisJBakke Bravo sir. I tried my own attempt at this yesterday but I am humbled by your artistry.
English

Just walked in the front door after work.
My 5 year old son ran to greet me.
"Hi dad!" he said excitedly.
As he went to hug me, I grabbed his shoulders and said, "Bud, I think you're overestimating the value of human relationships. I read that in a Substack today. Everything is different now. I mean - it was different before, but it's super different now."
He blinked, clutching a plastic dinosaur. I couldn't believe it. Attachment to physical objects in a post-digital era. I gently rotated him toward the hallway mirror.
“Look,” I continued, “do you see that reflection? That’s legacy hardware. Carbon-based. High latency. Limited processing power."
As I kicked off my shoes, my 3 year old daughter came running up to me with a drawing she made in preschool this morning.
She was glowing. Beaming.
“Look, Daddy! I made this for you!”
I glanced at it and explained that Nano Banana one-shotted her entire effort. Her job prospects were hopeless if she didn't understand this.
“Sweetie,” I said gently, kneeling down, “this crayon sun? It’s 2022. Nano Banana can generate 100,000 emotionally resonant suns before you finish saying ‘primary colors.’ You need API access.”
She asked what an API was.
“Exactly,” I said, standing up.
The crying started around then. Very emotional household. Understandable. They hadn't read *the essay.*
My wife heard the children crying in the foyer and came to check on us.
"I don't understand what's happening here, but why don't we sit down for dinner and talk about this?" she asked. "I made chicken pot pies!"
“Dinner? Your contribution to a world where Amex and Mastercard are heading to zero by 2028 is DINNER?!”
I started laughing.
“Uh yeah…” I explained: “Cooking is a pre-Claude activity. Do you realize I can vibecode a functional DoorDash competitor in about 8 minutes now? It's all right there in the Substack.”
As the kids continued sobbing, my wife looked at me in disbelief.
“Okay, okay. Maybe it would take me 15 minutes to spin up a functional Doordash competitor,” I conceded. “Payments integration can be annoying.”
She asked if I was feeling alright.
“Better than alright,” I said. “I’ve seen the roadmap. I've read the Substack.”
I gestured broadly at the house: “This? This is a future data center. The hugs? Deprecated. The drawings? Automatable. The chicken pot pies? Disrupted.”
My wife folded her arms. “You used to like chicken pot pies.”
“That was before I could prompt at a few hundred words per minute,” I said.
English
@SFGiants @sfgiantsmemes I think we are a victim of sfgiantscamps scam, spent $500 for my son's cancelled Oracle day camp in 2024 and we can't get refunded / it never happened due to "rain." Request refund, tix, and show at Currant Theatre. See you 3/13 in AZ.
English
Man I wish my investors would pump us on the socials like this
Chamath Palihapitiya@chamath
Everything about cancer sucks. Some of the most difficult decisions in cancer are what to do and when to do it: biopsy, resection, passive monitoring etc. Today, clinicians make irreversible calls like 1) do a biopsy or wait, 2) treat or monitor or 3) remove an organ or monitor, using tests that cannot see the full biology of either the body or the cancer. As a result, doctors often overtreat the wrong patients while missing dangerous cancers in others until it’s too late. Five years ago, a sibling trio of Purdue grads cold emailed me from Indianapolis. Their thesis was simple: the science in cancer detection and treatment isn't the bottleneck. The engineering is. Fix the engineering, and you can change the standard of care of cancer forever. We founded @EarlyIsGood together to do this. Here is our mid-decade update after five years (!) of toil. We’ve made some good progress. 1. The Engineering Unlock: Multiomics Most diagnostics fail because they are looking for a needle in a haystack. The results are modest and create many false positives and false negatives. We developed nanotechnology that amplifies the needle making it simpler for us to figure out what is going on. Our nanotechnology allows us to read DNA, RNA, and Proteins simultaneously from a single sample. We detect Proteins at attomolar sensitivity (1000x ELISA) and RNAs at PCR-level sensitivity all without extraction or amplification. Combining all three provides a full picture because: - DNA tells you what mutations are present - RNA tells you what the cancer is doing - Proteins tell you how the body is responding 2. The Proof: Bladder Cancer We started here because the standard of care today is barbaric. 800,000 people are under surveillance for bladder cancer, enduring invasive cystoscopies that still miss ~20% of tumors. We are finishing a multisite prospective trial now. Standard of Care (Cystoscopy): invasive, repeated every 3-6 months. Our bladder cancer test (BCDx): 92% sensitivity and 97% specificity from a simple urine sample. Most importantly, we catch the high-grade tumors that the current gold standard misses completely. 3. The Next Mountain to Climb: Prostate Cancer If you’ve watched a father, brother, or friend get a high PSA result, you know the spiral that follows: months of terror, invasive procedures, and paralyzing uncertainty. 20M+ PSA tests are run annually. Most positives are false alarms, leading to 1M+ unnecessary, painful biopsies. Meanwhile, dangerous cancers are often missed. Current commercial tests hover below 50% specificity. That means for every two men they flag, one is a false alarm. We partnered with the Mayo Clinic to solve this. No blood draws. No rectal exams. Just a simple urine test. We are using the same platform that we validated on bladder cancer to achieve unprecedented specificity without sacrificing sensitivity, effectively separating those who need treatment from those who don't. We will soon be commercializing both our bladder and prostate cancer tests widely. Follow us @EarlyIsGood if you’d like to help or know when/where these tests are available.
English
@stoolpresidente Dave been crashing out ever since he swung that hammer like he learned it watching a hallucinated AI YouTube instructional video
English

I’ll tell you this Stevie. 1. I would out trade you if I had your capital to start and #2 if I had your money this guy would 100% still be in a Mets uniform.
Steven Cohen@StevenACohen2
@stoolpresidente I love that idea , what a genius
English