Naka-pin na Tweet
Clara Text
55K posts


Clara Text
@Claratextet
"Eigensinn macht Spaß" Hermann Hesse "Mein liebster Zeitvertreib? Lachen!" Dalai Lama #GegenRassimusSexismus #GegenGewalt #GegenExtremismus jeglicher Couleur
Sumali Nisan 2017
791 Sinusundan683 Mga Tagasunod
Clara Text nag-retweet

Sonntag ist der „World-Hijab-Day“. Weltweit glauben Initiativen und Unternehmen, diesen Tag des Kopftuchs im Zeichen der Toleranz unterstützen zu müssen. Was Iranerinnen dazu zu sagen haben.
emma.de/artikel/nein-z…
#FreeIran #NoHijabDay
Deutsch
Clara Text nag-retweet

Dieser Qualitätszirkel wird von Sabine Maur beworben. Die Landespsychotherapeutenkammer Rheinland-Pfalz – dort ist Maur Präsidentin, nicht nur Vizepräsidentin – hat ihn extra zertifiziert. Für die Teilnahme erhalten Psychotherapeuten Fortbildungspunkte.


Deutsch
Clara Text nag-retweet
In Trans-Therapeuten-Kreisen ist das Verhalten weit verbreitet. Daher gibt Maur vermutlich auch so freimütig derartige Empfehlungen. Heike Zimmermann, die den „Qualitätszirkel” der DGTI für Psychotherapeuten moderiert, plauderte dazu bei anderer Gelegenheit aus dem Nähkästchen.
Deutsch
Clara Text nag-retweet

Auf der Webseite von @FrauenAktion werden Leserbriefe veröffentlicht, die die Presse ablehnt, hier @SZ.
Prostitution ist Verfügungsgewalt über die Frau (Zuhälter und Käufer) und Schuldknechtschaft, Tattoo des Besitzers inklusive.
#Prostitution
Frauen Aktion München@FrauenAktion
Hier ein weiterer unveröffentlichter Leserbrief; diesmal Silvia Reckermanns Reaktion auf einen Artikel der Süddeutschen Zeit zur #Prostitution. frauen-aktion-muenchen.de/leserbrief-an-… Wenn wir auch Eure unveröffentlichten Leserbriefe veröffentlichen sollen, mailt sie uns.
Deutsch
Clara Text nag-retweet

“Imagine going back to the 1980s, or even the 2000s, and telling people that in the future a trade union would actively seek to undermine the workplace rights of women. That it would slam nurses – nurses! – as ‘bigots’ because they would rather not undress in the presence of men. People would have called you a loon. Yet here we are.”
spectator.com/article/gender…

English
Clara Text nag-retweet

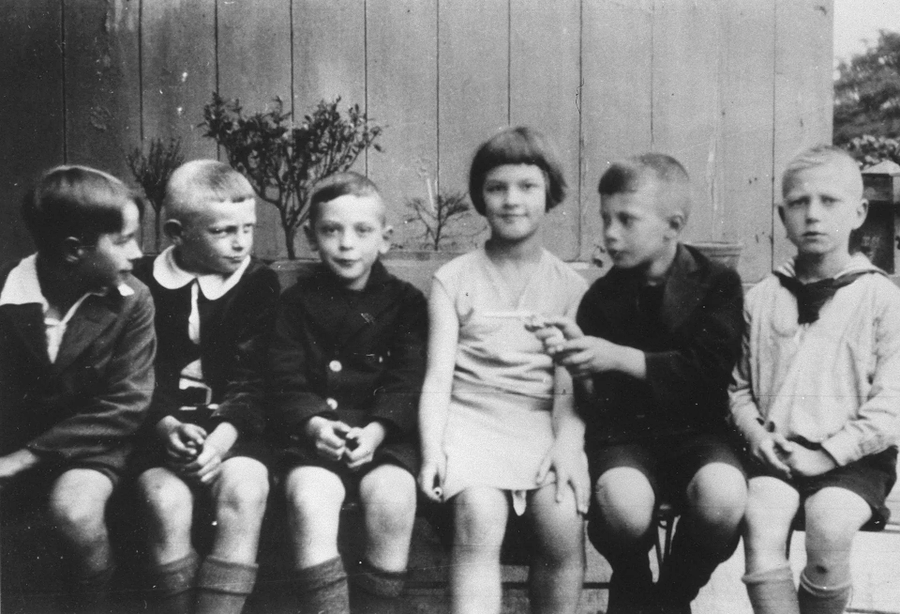
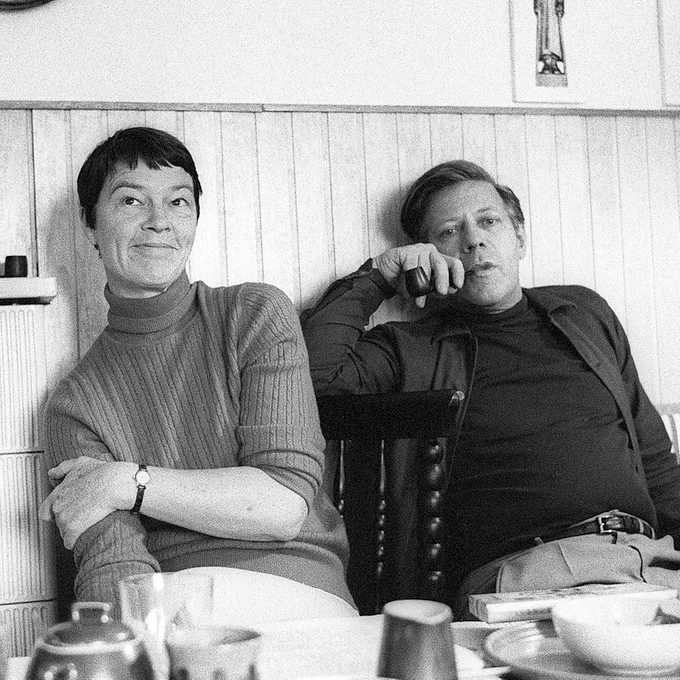
Loki Glaser, 1919 in eine Arbeiterfamilien geboren, wuchs in materieller Bescheidenheit und unbändiger Bildungslust auf.
Sie wurde Lehrerin, finanzierte ihrem Mann das Studium und bezeichnete sich selbst als "Angeheiratete der Politik".
#EducationDay #IhreSeitederGeschichte
Deutsch
Clara Text nag-retweet

Clara Text nag-retweet

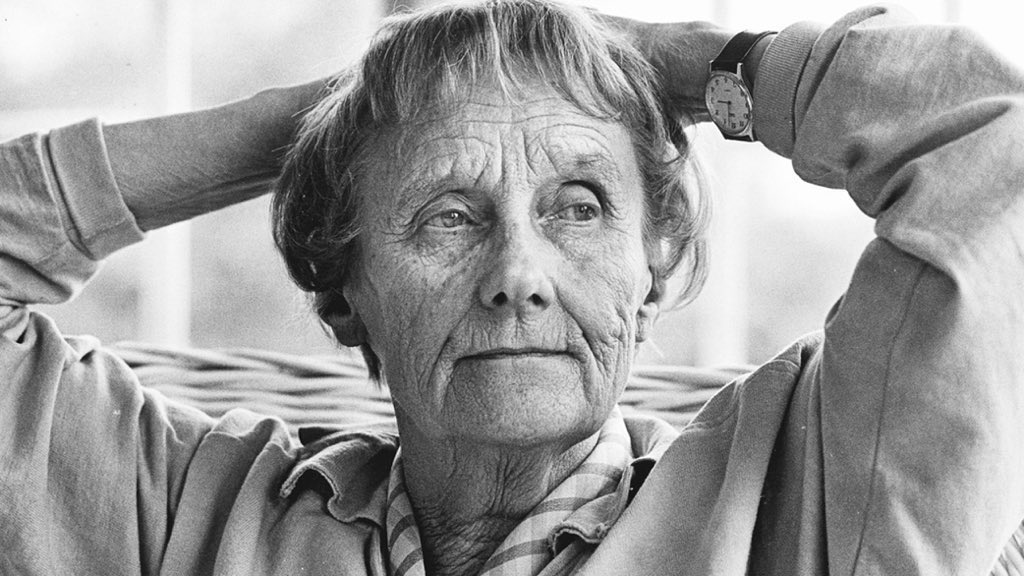
»Was der Sinn des Lebens nicht ist, das weiß ich: Geld zusammenzukratzen und solch eine Angst vor Einsamkeit und Stille zu haben, dass man nie in Ruhe über die Frage nachdenken kann:
Was mache ich mit meiner kurzen Zeit auf Erden?«
Astrid Lindgren,
gestorben am 28. Januar 2002
Deutsch
Clara Text nag-retweet

Gülden Hennemann warnt im Cicero-Podcast vor legalistischem Islamismus. Sie spricht über innermuslimische Ausgrenzung und Deutungsansprüche von Ahmadiyya, Muslimbruderschaft und IGMG sowie darüber, wie islamistische Milieus insbesondere seit 2015 durch Einwanderung aus dem arabischen Raum an Einfluss gewonnen haben – und warum der Staat diesen Entwicklungen bislang nur unzureichend begegnet.
ak-polis.de/guelden-hennem…
Deutsch
Clara Text nag-retweet

It is beyond time for everyone to learn that the LGB and the TQIA++ are very, very different things.

English
Clara Text nag-retweet

🚫 Stop using lesbians and gays to push ideological agendas! Read our statements opposing the proposed PACE resolution on “conversion practices”, and why extending these bans to gender identity does lasting harm in the name of human rights.
athena-forum.eu/updates/expose…
English
Clara Text nag-retweet
Welche Rolle spielen die EU und üppig finanzierte NGOs dabei, Transaktivismus in Gesetze zu gießen? Expertin und Gründerin des „Athena-Forums“ Faika El-Nagashi über die Hintergründe.
emma.de/artikel/die-ro…
@el_nagashi @AthenaForumEU
Deutsch
Clara Text nag-retweet

Mobbing
Jetzt auch ein Fall in Italien. Paolo war ein offensichtlich sensibler Junge. Er liebte die Musik, schrieb Tagebuch. Er hat die Musik aufgegeben, um in Mathematik besser zu werden.
Er wurde von vier Klassenkameraden gemobbt. Und was macht sein Lehrer? Stellt ihn vor der ganzen Klasse bloß und fordert ihn auf, sich zu prügeln.
Nach dem ersten Schultag nach den Ferien hat sich Paolo mit 14 Jahren das Leben genommen. Der Schulleiter wurde für drei Tage suspendiert, gegen die vier Klassenkameraden wird ermittelt. Eine weitere Ermittlung findet gegen Unbekannt statt, wegen Anstiftung zum Suizid.
Mobbing ist überall ein Thema. Gut, dass italienische und französische Medien das Thema jetzt aufgreifen.
RIP Paolo 🥀🪽🎸
Florinda Ambrogio@florindambrogio
“BULLIZZATO anche dalla prof davanti alla classe”, lo scrive nel suo diario Paolo Mendico, morto suicida a 14 anni. Il problema non è solo il #bullismo. Lo schifo è che questa insegnante, dopo un breve periodo di sospensione, continuerà a dialogare con adolescenti #giustizia
Deutsch
Clara Text nag-retweet


Clara Text nag-retweet

@KonradStockmei1 @cem_oezdemir @fdp #AusGruenden
Am 12.April 2024 hat die @fdp gemeinsam mit @diegruenen, der @spdde und @dieLinke im Deutschen Bundestag das Selbstbestimmungsgesetz beschlossen.
@BaWü

Deutsch



Offensichtlich haben noch immer zu viele den Ernst der Lage nicht verstanden. Europäische Souveränität muss sich im konkreten Handeln beweisen, die Zeit für wohlfeile Lippenbekenntnisse ist vorbei. #Mercosur (1/3)
Deutsch
Clara Text nag-retweet

@cynicalyetfun @fem_mb @ForWomenScot I'm so sorry. That's awful. I know it might not be much consolation, but I've come through this shitshow with a) more friends than I lost and b) a significantly higher quality of friend. May you be as fortunate x
English
Clara Text nag-retweet
I’m entitled to say this, because I just turned 60.
A lot of older liberals (in both the US and the UK) have brought very old-fashioned sensibilities to this debate. They’re still locked into the idea that all trans women are, or were, effeminate gay men, and they’re perplexed that any woman would see them as a threat.
These are people who’ve never met an AGP in the wild, don’t understand online cultures, know nothing about trends in porn, aren’t on TikTok where ‘gender-affirming’ surgeons advertise directly to minors, and they’ve aged out of having kids at school, so have no notion that social contagion might be at play. They look round at all their similarly aged dinner party friends, none of whom are aware of any of these things either, and adopt a vibe-based position: this is gay rights 2.0, anyone who opposes it must be far-right, and thank goodness Our Sort are kinder, better, and (most importantly) far more sophisticated.
English
Clara Text nag-retweet

Den Begriff "Genderidentität" gemeinsam mit „sexuelle Orientierung“ in Gesetzgebung "gegen Konversionspraktiken" zu packen, erweist nicht nur LGB einen Bärendienst, es knebelt Therapeuten, degradiert sie zu Erfüllungsgehilfen.
Hier der Brief eines Britischen Psychotherapeuten.
marcus evans@marcuse99903226
My letter to MPs concerning conversion therapy legislation I am writing to express serious concern about the unintended consequences of proposed further legislation on conversion therapy, particularly for legitimate exploratory psychological and psychotherapeutic work, which is fundamentally different from coercive attempts to suppress identity or deny genuine distress. I have worked in mental health services for over 45 years, including more than 20 years in senior leadership roles, during which I was part of and later ran the largest psychotherapy training and clinical department in the country. Throughout this long period of clinical practice, I did not encounter a single case of what is now described as "conversion therapy." What I have encountered repeatedly in recent years is something quite different: experienced clinicians becoming increasingly reluctant to work in this area at all. This reluctance does not stem from a lack of skill, care, or concern for patients, but from a toxic ideological environment in which freedom of thought is constrained and ordinary clinical exploration is readily misrepresented as harm. The result is a growing withdrawal of senior, experienced practitioners from precisely the area where thoughtful, developmentally informed clinical work is most needed. The consequences of this withdrawal are serious. When experienced practitioners step back, complex clinical work increasingly falls to less experienced therapists who may lack the authority or confidence to tolerate uncertainty. Under pressure, they can be drawn into polarised positions, affirming or challenging a patient's stated beliefs rather than supporting an understanding of the underlying psychological, developmental, and relational dynamics that drive the individual's attachment to those beliefs. This is not a failure of individual clinicians but of the environment in which they are expected to practise. These concerns were clearly reflected in the Cass Review, which noted that the environment surrounding the Gender Identity Development Service did not permit the usual open discussion, clinical challenge, and multidisciplinary debate that accompany services operating within a genuinely holistic model of care. Normal processes of reflection, disagreement, and clinical curiosity were inhibited, with serious consequences for governance and patient care. This was not an incidental failure but a systemic one. The ideological capture of clinical environments in this area has caused enormous harm. When particular beliefs become morally protected, clinicians are no longer free to consider the child in the broadest possible terms, developmentally, psychologically, relationally, and over time. Instead, fear of complaint, professional censure, or reputational damage supersedes clinical judgement. Safe and effective psychotherapy depends on clinicians working in environments that actively protect their capacity to think, question, and reflect without fear of recrimination. Without this freedom, clinical authority collapses and care becomes defensive rather than therapeutic. What distinguishes safe exploratory work from harmful practice is the freedom to think openly about the meaning of a patient's distress without predetermined outcomes, to consider multiple developmental and psychological factors, and to remain curious rather than directive. Several years before the Cass Review, I published an article in the British Journal of Psychiatry Bulletin titled Freedom to Think: The Need for a Thorough Assessment and Treatment of Gender Dysphoric Children (2020). The paper examined the ideological capture of gender services and the resulting erosion of the freedom of thought required for safe and effective clinical practice. It became one of the most widely downloaded articles the journal has published, reflecting how widely these concerns were already shared among clinicians. The Cass Review's subsequent findings confirmed many of the issues raised. More recently, in my paper Beyond Affirmation: Lessons from Tavistock's GIDS, I reflected on how clinical authority within the service progressively collapsed as the affirmation model was used to avoid the painful psychological work of exploring a young person's underlying conflicts and motivations. Rather than supporting clinicians in asking fundamental questions about who this child is, what their distress means, and how their history, relationships, and internal world shape their beliefs, affirmation increasingly became a defensive response to institutional anxiety. This foreclosed the development of a genuinely holistic clinical picture and narrowed care to the management of identity claims rather than understanding the person. Since 2019, my wife, Susan Evans (who was the first whistleblower in 2005 and took the judicial review with Keira Bell), and I have received, on average, several letters each week from parents concerned that their child's pre-existing psychological and developmental difficulties are being overlooked, while services and associated charities encourage the child to view transition as the primary solution to their distress. These parents consistently emphasise that they are not opposed to transition in principle. Their concern is that, given their child's history of anxiety, trauma, neurodevelopmental vulnerability, or social difficulties, these factors have not been sufficiently explored before the child is placed on what they experience as a fast-tracked pathway towards a medicalised approach. Parents express fear that this approach, which has never had a robust evidence base, risks bypassing underlying psychological difficulties and may lead to regret that could have been avoided through more careful assessment and understanding. In our clinical work, Susan Evans (Psychoanalytic Psychotherapist) and I have also found that many children and adolescents presenting with gender distress experience profound self-hatred and a markedly limited capacity to see themselves as complex individuals developing over time. Their distress is often organised around a concrete, punitive view of the self, leaving little room for curiosity or symbolic understanding. With careful psychotherapeutic support, many gradually begin to reflect on themselves, understand their feelings and histories, and consider the nature of their own minds. As this reflective capacity develops, the pressure for dramatic, body-based solutions to psychic pain often diminishes. Instead of seeking to escape distress through irreversible interventions, these young people begin to experience themselves in more nuanced, humane, and psychologically flexible ways. There are therefore significant clinical shortcomings in the current affirmation-led model of care that further legislation risks reinforcing. An approach that prioritises affirmation as a default response can overshadow underlying psychological, developmental, and relational difficulties that are often central to a young person's distress. When exploration is foreclosed, opportunities for understanding and effective treatment are lost. It is also essential to recognise that identity development, particularly in childhood and adolescence, is a process rather than a fixed state. Adolescence is characterised by uncertainty, experimentation, and change as young people work through questions of self, body, sexuality, and belonging. Psychotherapy supports this process by helping individuals understand themselves, their motivations, and their attachment to particular beliefs, enabling them to make informed decisions over time. It is not about converting patients to a therapist's view of who they should be. Further legislation in this area will therefore likely deter experienced clinicians from undertaking work that is already highly pressured and morally charged. The effect will not be increased safety but a further thinning of expertise, leaving vulnerable individuals with fewer opportunities for thoughtful, experienced psychological care. What is needed instead is strong clinical governance, clear professional standards, and institutional support for reflective practice, rather than further legislation that risks criminalising ordinary therapeutic thought. Yours sincerely, Marcus Evans Marcus Evans is a consultant psychotherapist and Fellow of the British Psychoanalytic Society. He worked for over three decades at the Tavistock & Portman NHS Foundation Trust, where he served as Associate Clinical Director of Adult and Adolescent Services and as Head of Nursing and Professional Discipline. During his tenure at the Trust, he was appointed a governor with specific oversight of the Gender Identity Development Service (GIDS). He resigned from this role in 2018 due to concerns about the clinical approach and governance failures within the service. He was among the first senior clinicians to raise concerns publicly about GIDS and has published extensively on gender distress, institutional dynamics, and the conditions required for reflective psychological care. @wesstreeting @NHSEngland @CareQualityComm @rcpsych @BPSOfficial @SexMattersOrg @genspect @AthenaForumEU @RosieDuffield1 @sharrond62 @SexMattersOrg @JournalismSEEN @Transgendertrd @sueevansprotect @genspect @ClaireCoutinho @Hilary_Cass
Deutsch
@UserUswr54069 @againstgrmrs @PoliticalMixter Apropos "wes Geistes Kind":
Es gibt eine Ärztin, die ihre Approbation in UK verloren hat und verantwortlich für viele Einzelschicksale ist.

Deutsch

@Claratextet @againstgrmrs @PoliticalMixter Ich bin selbst Betroffene und kann sehr wohl unterscheiden, wessen Geistes Kind Jemand ist
Es ist meine Meinung und sie können meinetwegen weiter Lügen glauben
Es gibt keine Ideologie, sondern viele Einzelschicksale
Deutsch

SO 👏 ARE 👏 WE 👏
It is truly evil to tell children that they were born wrong.
There is no wrong way to be a boy or girl. No child is trans.

English