Meroka
231 posts


Meroka
@JoinMeroka
Restoring humanity in healthcare by helping physicians lead with purpose, autonomy, and connection. #IndependentMedicine
شامل ہوئے Haziran 2022
80 فالونگ60 فالوورز
@6_BurghSteelers @Cigna This is the system working exactly as designed. Deny, delay, exhaust — until you give up or pay out of pocket.
English

The missing piece in most AI pricing conversations: who owns the care relationship matters. If AI-powered care flows through PE-owned or corporate systems, pricing will optimize for margin. If it flows through independent, physician-owned practices, pricing can actually optimize for patients. That's why we're building Meroka.
English

How should care be paid for in a world of abundant supply and consumers continuously engaged with AI-powered clinicians? Hundreds of AI pricing experiments are playing out in the wild as we speak, including CMMI leading the charge through ACCESS. Looking forward to discussing the state of the state and where this is all headed with my friends Rohit Chandra of @ClevelandClinic and @AbeSutton of CMMI at ViVE. #ViVEvent

English
@HealthcareAIGuy VCs see health AI as a goldmine. Who pays? Physicians, with their autonomy chipped away. The system wins again.
How to fix that?
English

@LeahHoustonMD Agreed. Tech should augment, not replace, the physician's judgment. The human connection is foundational to good medicine...
English
@LeahHoustonMD @Innovate_FB @martinamps Cash is the way. Well, in the US at least. Bypass the prior auth rage, the denials, the paperwork tax. Lets you take back control...
How can physicians increase cash-pay services while still lowering costs for patiens?
English

@Bob_Wachter @dpatil @cwclub @Bob_Wachter Always fascinating to hear how data can fix a system that seems determined to break itself. Good stuff. Thanks for sharing!
English
My far-ranging and fascinating interview with health tech expert and entrepreneur (and former chief data scientist of the U.S.) DJ Patil (@dpatil) at the Commonwealth Club @cwclub.
youtube.com/watch?v=bXZv-Q…
YouTube
English
@mcuban @HammondOnHealth Preach!!! And when docs consolidate under hospital systems, insurers get to negotiate even *lower* rates. Independence is the only leverage left.
English

If insurance companies paid indie docs a fair wage rather than underpaying , late paying and auditing them to clawback as much as they can, the rest wouldn't matter. The docs could be profitable. ..this is not new. The insurers do the same thing to indie pharmacies via their PBMs
English

I'm supposed to cheer when gov't claims it has a solution to the problem it created? We're propping up a rotting foundation by piling more on instead of fixing it. This doesn't address the cause of the problem & based on the history of the banking & oil industries, it won't work.
Mark Cuban@mcuban
Great job @HawleyMO & @SenWarren LOVE THIS. Anyone in Congress that doesn’t support this, doesn’t want lower cost healthcare for Americans. This is a no brainer. Let’s hope @POTUS puts his weight behind this
English

There’s a strange disorientation when the thing that once earned respect starts raising concern instead. When someone says they worked through the night, the room no longer nods automatically. — article written by The SoMeDocs Team doctorsonsocialmedia.com/the-badge-of-h… via @somedocs
English

I interviewed a psychiatrist, a clinical psychologist, and a physician advocate who are challenging the idea that medicine must be miserable.
Dr. Sarah Hollander, Dr. Kelly Holder, and Kim Downey joined me to discuss why we need to build a new culture of "joy in medicine."
They argue that joy is not just a fleeting emotion or toxic positivity. It is a value system that can anchor us through the hardest days.
Dr. Hollander pointed out that the current medical system often mistakes endurance for excellence. We praise grit and suffering, but endurance without balance feels like constriction and shame. Joy, on the other hand, feels like expansion. It is a "pulling" sensation toward a calling, rather than a "pushing" sensation against resistance.
So how do we operationalize this?
For Medical Students: Stop asking them what specialty they want to do based on prestige or expectations. Ask them what lights them up. When a student talks about a topic that makes their whole body change, that is their joy. Follow that.
For Attendings: Share the reality of the work, including the struggles. Joy isn't the absence of pain; it is the presence of community. When we hide our challenges, we isolate ourselves. When we share them, we build the connection that sustains us.
Kim Downey emphasized that these "soft skills" are actually foundational for patient safety. A team that feels a sense of belonging communicates better, makes fewer errors, and provides better care.
Joy is not a luxury. It is a necessity for a sustainable healthcare system.
🎙️ Listen to "Is joy in medicine a new culture?" on The Podcast by KevinMD.
📷 Search "The Podcast by KevinMD" on Apple or Spotify.
#KevinMD #JoyInMedicine #PhysicianWellness #MedicalCulture #HealthcareLeadership #BurnoutPrevention #HumanismInMedicine

English
Meroka ری ٹویٹ کیا

$275 billion.
That’s how much the federal government takes from hard working Americans and hands to hospital systems every year in subsidies, tax breaks, and payment advantages.
Independent physicians receive $0 of it.
The Break Up Big Medicine Act touches $0 of it.
Not a coincidence.
Warren and Hawley love the American Hospital Association.
And where are the @GOPDoctors?
Nowhere.
English
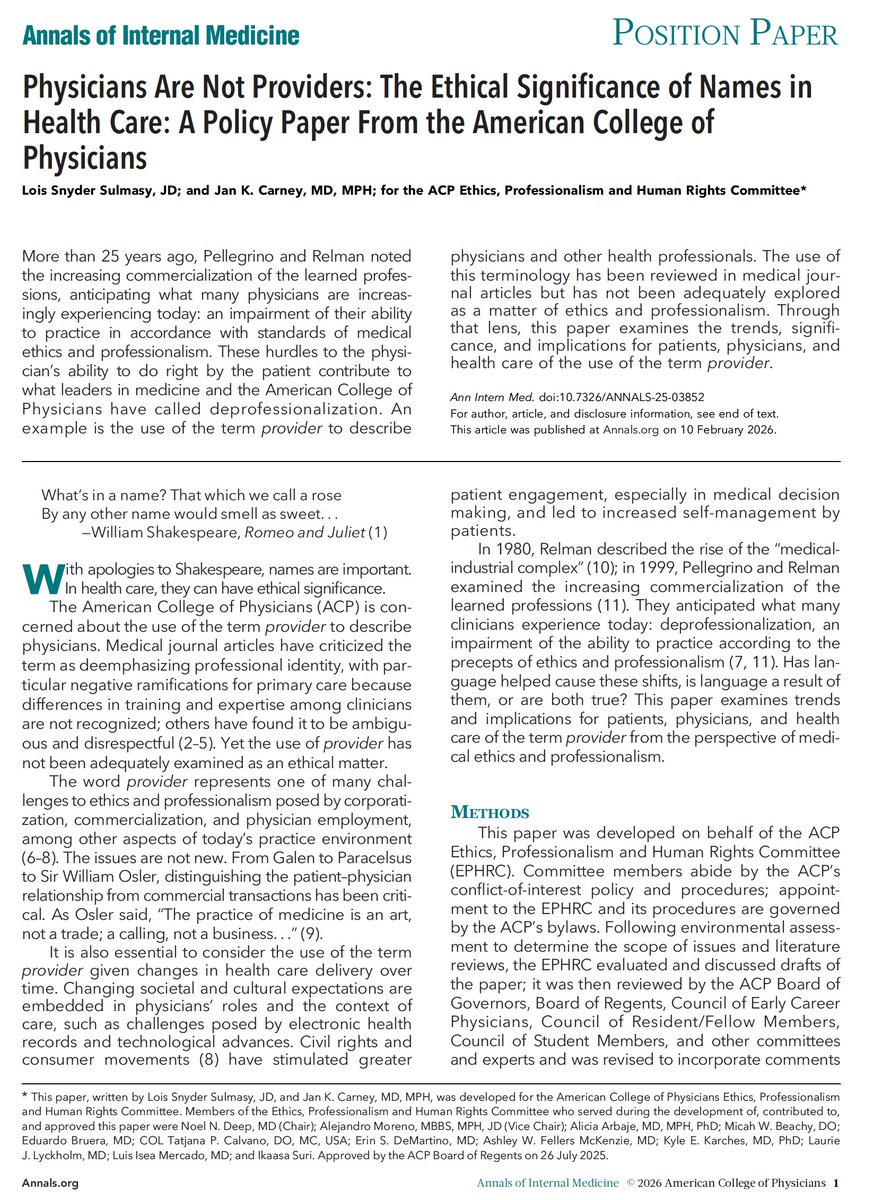
@EricTopol @AnnalsofIM @ACPIMPhysicians The whole system isn't broken. It's working exactly as designed - replace physicians with "providers", patients with "customers" and you get a system that values "profits" over health.
English

"The term [provider] should not be used to describe physicians, nor should physicians use it to describe themselves, their team members, or their trainees."
acpjournals.org/doi/10.7326/AN… @AnnalsofIM @ACPIMPhysicians
English
@SpineNeuro The system isn't broken. It's working exactly as designed. To put money in health oligarchs, and out of physicians and patients.
English

🎯the health oligarchs cannot control docs without demoting us to “providers”.
Look at the websites of major health systems like Kaiser , you will notice they have no names or profiles of doctors .
We are being erased to maximize healthcare power and profit .
Wesley J. Smith@theWesleyJSmith
The term is part of deprofessionalizing medicine and turning it from a "practice" into a technocratic trade in which the customer orders what he or she wants and the doctor provides.
English

AI is about to fix one of medicine's most well-intentioned but potentially dangerous practices. The chart biopsy.
Before seeing a patient, a doctor is going to do their best to review the chart so that they have the context needed to handle whatever the patient's chief complaint is at the time effectively. Oftentimes, doctors do not have time to review the entire chart or review the chart at all, secondary to the ongoing pressures to see more and more patients.
The very best doctors I've known have, at the very least, tried to do a chart biopsy. They scan through the available previous documentation in the chart and try to intelligently choose pieces of documentation that are likely to provide them with a good overall picture of the patient. For example, a previous specialist note.
The reality is that they can only choose one or two notes to read—hence the term chart biopsy. Just like a real tissue biopsy, it is only taking a tiny sample of what is going on. A good chart biopsy is better than no chart review, but it leaves a tremendous amount of unreviewed context.
In the course of an inpatient hospitalization, as the hospitalization plays out, a great doctor will review more of the chart through those days and learn more about the patient. They accumulate previous context and present context through their conversations with the patient over time.
But at the time when they are seeing the patient and admitting the patient and making the most critical decisions, they often have the lowest context.
Growing context windows mean that an AI can actually process more text than the average human can. A million token context window is the equivalent of about ten novels. For patient records that are even bigger than this, they can be represented and searched using techniques including context compaction, summarization, and vector embedding.
AI is going to make it so that the chart biopsy is not necessary. We are going to have considered all the available context early on in patient encounters, at the point of care when it really matters. This is going to help doctors be more effective at their job of diagnosis and treatment planning, and lead to downstream positive impacts for patients.
English
@realdocspeaks We are tech bros who understand healthcare, and this is exactly what we are doing!
English
Everyone's betting on the game tonight. Meroka's betting on independent medicine's comeback in 2026.
#SuperBowl
English
Football team: 53 players, everyone knows their role.
Healthcare system:
Patients think they're covered (plot twist: you're not)
Physicians want to treat you (insurance says no)
Nurses trying to keep it together (with half the staff)
Administrators and insurances (the only ones scoring)
System working exactly as designed. Just not for the people in the game.
#SuperBowl
English